On 16 April Baroness Hallett published her report on the Vaccines and Therapeutics programmes following on from public hearings held in the early weeks of 2025. The overall message is that the programmes were a success, but there were also problems . Many of the issues encountered by clinically vulnerable families are picked up in the report, if not in the headline messages, but some points are missing. This is discussed further in a blog from Lara Wong, Head of CVF (clinically vulnerable families). In addition, on publication day several members of the CVF group took the high profile opportunity to explain the issues on live TV.
Key Points from the Module 4 report
The headline message from the report is captured in the opening paragraph of the summary:
‘The UK authorised and delivered effective vaccines and therapeutics to the public within a year of the first identified case of Covid-19 in the UK in January 2020. One of the vaccines had also been developed in the UK’.
The report goes on to conclude that the achievements showcased many of the best attributes of the UK’s health and scientific research systems. Key elements of the UK response that enabled it to to develop or discover effective vaccines on this speedy timetable were :
- the rapid and coordinated funding for research into vaccines and therapeutics;
- an expedited regulatory approval and recruitment system for clinical trials, as well as expedited authorisation of new vaccines and therapeutics, without compromising on public safety;
- the rapid establishment of specialist vaccine and therapeutic taskforces, which brought together national expertise and acted decisively to coordinate the search for effective vaccines and drugs;
- the adoption of an at-risk approach to vaccine procurement by funding research on and development of a wide range of vaccine candidates, knowing that some would not be successful, to create as many opportunities as possible to discover an effective vaccine.
However, the report caveats this by also concluding :
‘The UK was in some ways fortunate that the timing of Covid-19 coincided with the coming to fruition of decades of global research about technologies that could quickly be adapted and used to create vaccines. ‘ And
‘In relation to therapeutics, preparedness was focused on stockpiling of anti virals for an influenza pandemic. ‘This focus on influenza is of course also picked up by previous reports from the inquiry.
Baroness Hallett also concludes that the UK entered the pandemic without sufficient drug and vaccine manufacturing capability – something that needs to be addressed. She also notes that it is also vital to continue investing in the UK’s research and development capabilities, and to maintain robust regulatory systems for authorisation and post authorisation.
According to the report the delivery of vaccines was a success, but it did not deliver effectively for all groups in society. For example, there were problems in delivery to and take up of vaccines in communities with the greatest levels of deprivation and amongst some ethnic minority populations.
Vaccine hesitancy is of course on the rise and misinformation across social media platforms is a key conduit for the spread of this . The report stresses that the UK must take action to build confidence in vaccines before the next pandemic.
The inquiry makes five key recommendations as follows:
- establishing a pharmaceutical expert advisory panel to oversee the UK’s preparedness to develop, procure and manufacture pharmaceuticals (vaccines and therapeutics);
- producing targeted vaccination strategies and communications in order to increase vaccine uptake and reduce inequalities, including consulting with local networks about communication campaigns and delivery approaches;
- improving monitoring and evaluation of vaccine uptake and delivery in order to understand the measures proven to be effective in increasing vaccine uptake;
- facilitating regulatory bodies’ access to healthcare records for the purposes of post-authorisation safety monitoring of new vaccines and therapeutics; and
- reforming the Vaccine Damage Payment Scheme as soon as possible, with an increase in the minimum payment awarded to those injured by a vaccine and a fairer system for determining payment.
Clinically Vulnerable Families
In my assessment the tone of the headline message is a touch over positive. Yes, in many respects the vaccine programme was very impressive and saved hundreds of thousands of lives , but below the surface it did not always deliver for clinically vulnerable people nor for other groups.
I would also conclude that the therapeutic s programme was even less of a raging success given many CV people were unable to take the vaccine and often left without effective treatments and protections. Similarly people for whom the vaccine offered little in the way of protection were left without any form of protection.
This relatively neglect of therapeutics is endorsed by the chair of the vaccine task force, Kate Bingham who referred to it being manifestly wrong – both morally and ethically. During the Module 4 hearings Bingham was forceful in making it clear that therapeutics received lower priority and the programme was not characterised by the ‘vim and vigour’ of the vaccine programme – see my previous blog. This is something that is acknowledged by a number of people, yet this is not a headline in the report.
Evusheld
A key issue to emerge, particularly for severely immunocompromised patients was the lack of prophylactic drugs to help protect them from catching Covid. Yet there was a drug available which would have allowed these people to stop shielding when society opened up. The drug Evusheld was available in most other developed countries but the UK refused to buy it and it is clear that the decision not to buy it was taken on cost grounds.
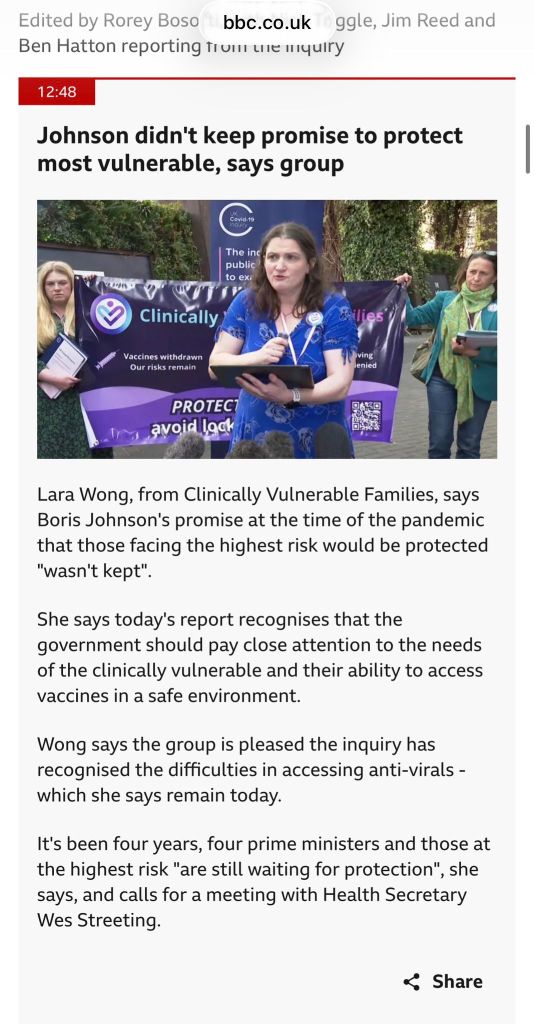
Baroness Hallett acknowledges that many of those who were not protected by the vaccine during the pandemic felt left behind and she quotes directly, from Lara Wong’s oral evidence:
“[Evusheld would have given severely immunosuppressed people] the freedoms that other people received through their own vaccination, and the consequence of not protecting this group was phenomenal in terms of their mental health, in terms of their social connections, in terms of their general ability to re-engage with the rest of the world.” Lara Wong, Founder of Clinically Vulnerable Families
Hallett goes on to conclude:
‘Evusheld may or may not have been the answer, but the Inquiry accepts without reservation that the need to provide protection to the immunocompromised, including through prophylactic drugs, must be a priority when preparing for the next pandemic.” Module 4 report para 3.93
This is a significant recommendation and in my view it should have been included in the headline recommendations.
As with many of the other key points made by CVF , they are in fact picked up and acknowledged in the report and there are a range of helpful recommendations, but they have not been drawn out as headline messages.
The rest of this sub section discusses antivirals; portfolio of treatments; safety at vaccine sites, vaccination of children; NHS records. Finally I briefly discuss the current problem of the ever narrowing criteria on who is entitled to a free vaccine booster.
Antivirals
Anti virals are drugs taken after someone has tested positive for Covid in order to protect those at risk due to clinically vulnerability from becoming seriously ill. They usually need to be taken within 5 days of someone testing positive.
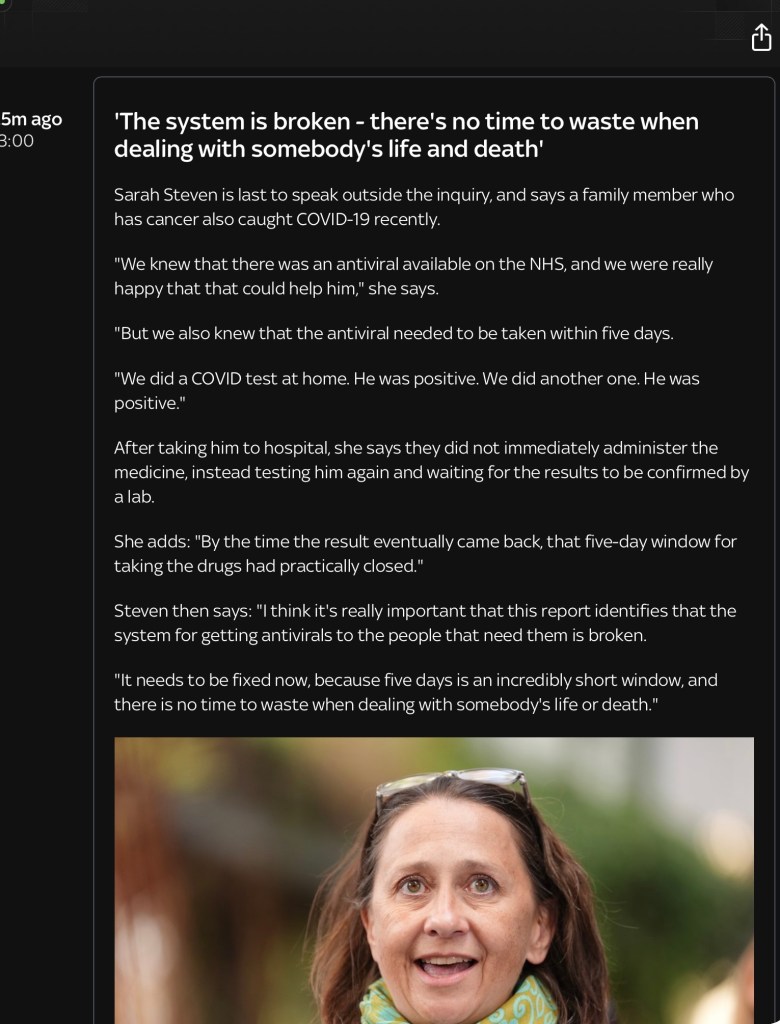
Whilst the system for allocating anti viral drugs may have looked fine on paper, the actual delivery was completely chaotic. The eligibility lists for antivirals were confusing and different from priority lists for people entitled to booster doses of the vaccines. Whilst some people, including my husband, received a letter saying he was eligible many others did not. On top of this many clinicians did not know who should be receiving anti virals and a common experience of CVF members was to be passed from pillar to post trying to obtain them – from GPs to 111 and back again, then to hospitals, all whilst the 5 day clock was ticking. In many cases the time period in which antivirals would be helpful elapsed whilst people were frantically trying to obtain them. In the section below on Positive Media coverage for CVF, CVF member Sarah Steven told the press about the experiences of a family member in trying to obtain antivirals.
As is clear from Lara Wong’s blog many doses that were purchased were never used and ‘the Treasury’s own closing submission revealed that nearly 5 million doses of anti virals were binned- not because there was no need for them, but because the system could not deliver them to the people they were bought for.’
It is encouraging that Baroness Hallett recognises the challenges and problems in her report. Indeed the report states that in any future pandemic, “messaging in relation to eligibility for therapeutics and antivirals and the extent to which this might differ from other criteria or lists should be clear and easily understandable.”
However, as Lara notes in her blog, this is not the overhaul of the antivirals pathway our members need, but it does at least acknowledge something CVF have been raising for years – that the eligibility lists for vaccines, boosters and antivirals were different, confusing, and frequently changed. People who were entitled to treatment did not know they were entitled, and even clinicians frequently did not know.
Safety at Vaccine Sites

People’s experiences of vaccination centres were very different. Some people, including myself, were fortunate to attend a large well organised venue at a race course with very high ceilings and a generally well ventilated feel. Others had to crowd into cramped badly organised stuffy venues with very little mask wearing and many CVF members said that attending sites to get the vaccine felt unsafe. There was often scrupulous attention paid to washing chairs at regular intervals despite the fact that it was well know by this point that Covid 19 was an airborne virus and not something that could be combated simply by cleaning surfaces.
It is reassuring that the module four report acknowledges that future systems of vaccine delivery must “pay close attention to the specific needs of the clinically vulnerable, to ensure that they are able to access the vaccine in a safe environment.”
Vaccination of Children
As Lara’s blog makes clear, ‘families with a clinically vulnerable member or where a child was CV were desperate to return their children to school safely’. But the UK’s vaccine offer to children was too slow, too limited, and too short. It was and is to this day markedly out of step with comparable countries including the United States, Canada, and Europe.
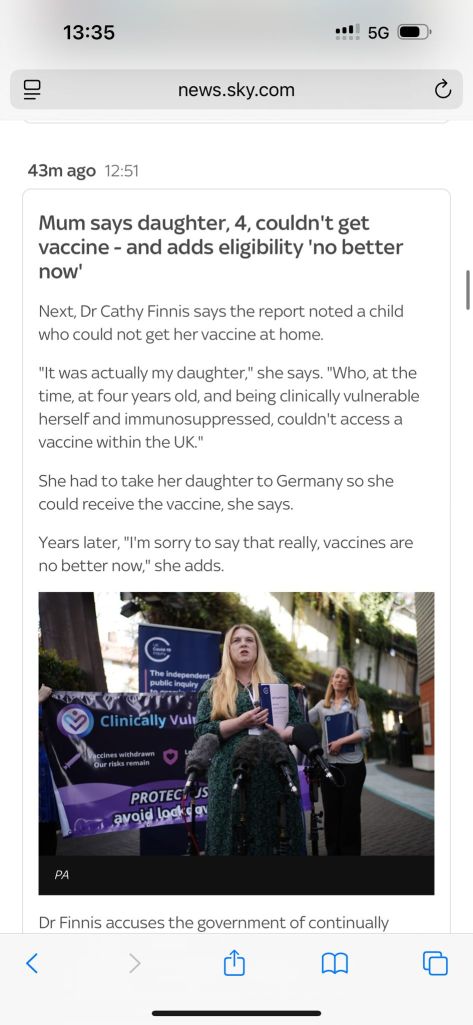
One of the roles of CVF during this period and indeed now was to encourage members to share information about accessing children’s vaccines abroad. Germany, was the most popular location and many CVF members have travelled multiple times to fully vaccinate their children. See for example the clip from the next section of CVF Deputy Cathy Finnis talking about travelling to Germany to get her child vaccinated.
As Lara notes, the report’s findings on children’s vaccines are less positive than hoped. We need to keep lobbying as our families should have a choice. This should include access to private vaccines since it is impossible to get a child under 12 vaccinated in the UK.
Access to NHS records
Many of the problems encountered in, for example, determining who should be eligible for antivirals, vaccine priority and eligibility lists etc stem from poor NHS records that make it impossible to get a complete picture of patients and their illnesses in one place. As noted by Lara Wong, ”CVF’s members have lived for years with the consequences of fragmented healthcare data. Many people were missed off priority lists because their codes were not linked. Some people’s eligibility for antivirals was effectively invisible because their GP and specialist care records weren’t connected. Disappointingly, Professor Sir Chris Whitty told the Inquiry that the UK has actually “slipped backwards” on linking data together since the pandemic.’
Baroness Hallett acknowledges the problem and her recommendation is strongly welcomed.
Recommendation 4 of the report calls for the MHRA to be granted “specific and proportionate access to comprehensive and comparable data from across the four nations of the UK, including linked primary and secondary healthcare data records”, with strong safeguards for patient confidentiality overseen by the Information Commissioner’s Office.
Positive Media Coverage for CVF
Through careful planning and media handling the CVF were highly successful in getting our message across on module four publication day as illustrated by the following clips of live news coverage on Sky News and the BBC.
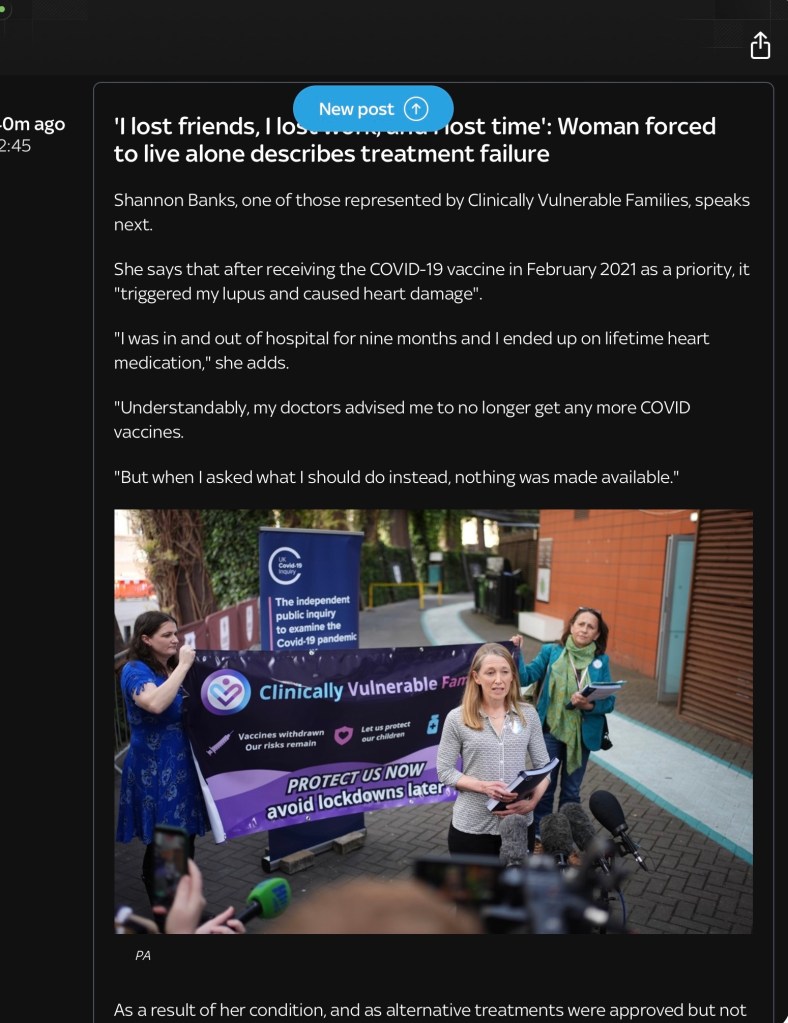
The success of CVF in getting the message across is further illustrated in the various news clips that ran throughout the day. The team are to be congratulated.
The Current Situation regarding Vaccine Boosters
Finally it is worth mentioning that the list of people entitled to a free nhs Covid booster has become narrower and narrower over time. This important issue is out of scope of the Covid Inquiry which only considers the period up to mid 2022, but it is highly relevant to the subject matter of the Inquiry and of critical importance to CVF.
The current situation is that only those living in care homes for the elderly, those over 75 years old and certain immunosuppressed patients are entitled to free NHS boosters. I estimate that the majority of CV people and even some people previously deemed clinically extremely vulnerable are no longer eligible. This includes cancer patients, those with heart conditions, kidney disease, severe asthma and neurological conditions. Even I am not entitled to the vaccine despite having bulbar onset motor neurone disease and being assessed as needing close monitoring by a leading centre in the treatment of complex respiratory failure. I had to pay for a booster last autumn but by careful planning and framing of requests I recently found a friendly professional willing to skirt round the rules and give me a free booster. This took know how and determination but we should not have to go to these lengths to protect ourselves.
The recommendations to government on who should be eligible for a Covid-19 booster are made by the Joint Committee on Vaccines and Immunisation (JCVI). There is a great deal of disquiet amongst experts about how the committee works. Moreover, the basis for their recommendations are far from transparent. Nevertheless all of the committees recommendations on Covid boosters to date have been accepted in full by various governments.
In my assessment there are numerous flaws with the underlying work done by the JCVI, the underlying analysis and data for which has never been published. In particular, the JCVI ignores the evidence that Covid-19 remains a significant threat to the health of people, including those with severe respiratory diseases, autoimmune disorders, cardiovascular conditions, and other chronic health issues.
A key drawback is that the JCVI base their recommendations solely on modelling of how many deaths and hospital admissions would be prevented by implementing various eligibility criteria for free boosters. This seems to be entirely driven by a cost – benefit analysis (kept secret) couched in purely financial terms. They are not saying it will prevent all deaths or admissions. But this is an incomplete picture of the costs as the JCVI work takes no account of the extra pressure on the primary healthcare system – that’s GP practices, urgent care centres and A and E departments of already seriously ill people coming forward suffering from Covid-19.
This focus is on very narrow criteria of preventing hospitalisations and deaths also means that the JCVI ignore the wider range of health, social and economic benefits (eg sickness absence, withdrawal from the labour force) of vaccinating a bigger percentage of the population. It is true that the scientific community are divided on the question of whether boosting people reduces transmission of the virus – but there is high agreement on the point that boosters reduce the chances of becoming seriously ill with Covid-19.
Other key flaws in the JCVIs work include ignoring the benefits to babies of vaccinating pregnant women (also resulting in savings to the NHS), and the lack of acknowledgement of the role of vaccines in preventing Long Covid., The JCVI also ignore the issue of how Covid-19 transmits and the potential benefits of vaccines in reducing transmission which could benefit schools, hospitals, reduce NHS staff absence as well as bringing numerous other benefits (see my previous blog).
All of this means that the direction of travel really needs to change before this year’s Autumn booster programme is announced. Whether this happens will of course depend on the outcome of the current political turmoil discussed briefly below.
Concluding Comments
The final report of the Inquiry is not due until next year and there are a further six module reports scheduled to appear before then. Given that many of the important points raised by CVF during module 4 are captured the detailed, rather than the headline conclusions and recommendations, there is a danger that they will get overlooked when drawing up the final report. It is important to do everything possible in the way of continued lobbying and publicity to prevent this from happening.
The UK government is, of course, currently in a state of uncertainty and potential flux. Against this backdrop it is unclear how far the recommendations of the Inquiry will be implemented, and whether this will be done with sufficient determination and energy. I do not have a crystal ball but as discussed in previous blogs it is up to key groups involved in the Inquiry and others, including academic experts, to keep all of this in the public domain and to keep pushing for change.
In the near term it is also unclear whether there will be attempts to further narrow the list of those entitled to a free Covid vaccine booster. Given the strength of the case for extending rather than further narrowing the criteria, we can but hope that some future Secretary of State for Health sees sense and at least brings the criteria for Covid jabs into line with that for the annual flu vaccination programme.
Gillian Smith 22 May 2026

Leave a comment