
In 2020 and 2021 the UK Government were keen to boost that they were world leaders in rolling out vaccination against Covid-19. It now seems like a very long time since those heady days of early 2021 when vaccination centres sprung up in the most unlikely of places across the country, staffed by NHS staff, former NHS staff and eager volunteers.
I received my first vaccination on a snowy day in February 2021 at the Epsom Downs Racecourse and can confirm the real sense of purpose amongst staff and volunteers, drawn mainly from the Jockey Club, to get people vaccinated and get the country back on its feet.


At the time most people thought that was it – we had won and we would defeat the virus and that we would all be able to access the vaccine in future if things began to take off.
Sadly, this has not proved to be the case. As societies have opened up the virus has shown an incredible ability to reproduce itself and mutate in multiple ways that it is acknowledged that we have never seen before.
Vaccine manufacturers have struggled to keep up with it to the extent that it is acknowledged that being vaccinated will not necessarily stop you from catching Covid, but it is likely to keep you out of hospital and prevent you from dying. However, this is not the case for everyone, particularly the clinically vulnerable, including a member of my household, who have failed to produce antibodies from the vaccinations and booster jabs.
This blunting of the severity of the virus is in part at least where the myth that the virus is now mild and can be treated much like flu or even a cold came from. And partly in response to this ‘it’s mild’ narrative, the take up the vaccination has also declined over time, even when people are eligible.
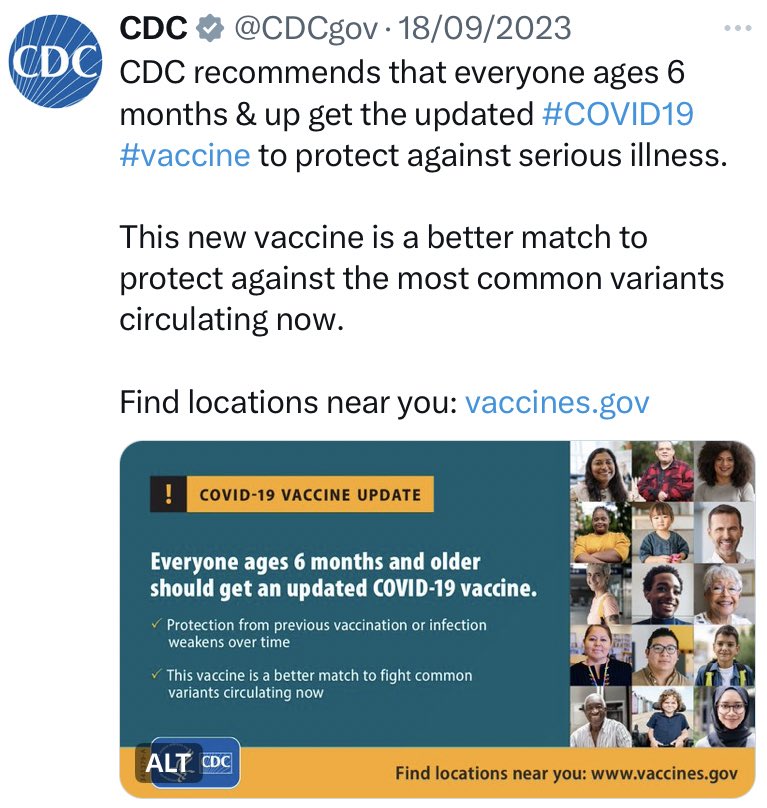
In parallel to this narrative, eligibility for vaccine boosters has become narrower and narrower over time to the extent that the UK now lags seriously behind other western countries. In the UK this winter the booster jabs are only available to the following groups (diagram on left). This is in sharp contrast to the US and Canada where anyone over 6 months can get a jab (photo on the right relates to the USA).

UK Vaccination Policy Autumn 2023
The rest of this blog drills down and discusses what this narrowing policy is based on.
It is the job of the Joint Committee on Vaccination and Immunisation (JCVI) to advise the government and their recommendations tend to be accepted not least because they operate very closely with the UKHSA, indeed there are several members of UKHSA on the committee. (UK Health and Security Agency headed by Jenny Harries).
What has happened last spring when the JCVI drew up its recommendations is very strange, particularly when one considers that the government had already bought enough vaccine to vaccinate the same cohort as last year, as is evident from the paragraphs below, drawn from annex 1 of the government document, and which I am grateful to the Cat in the Hat twitter account for pointing out.
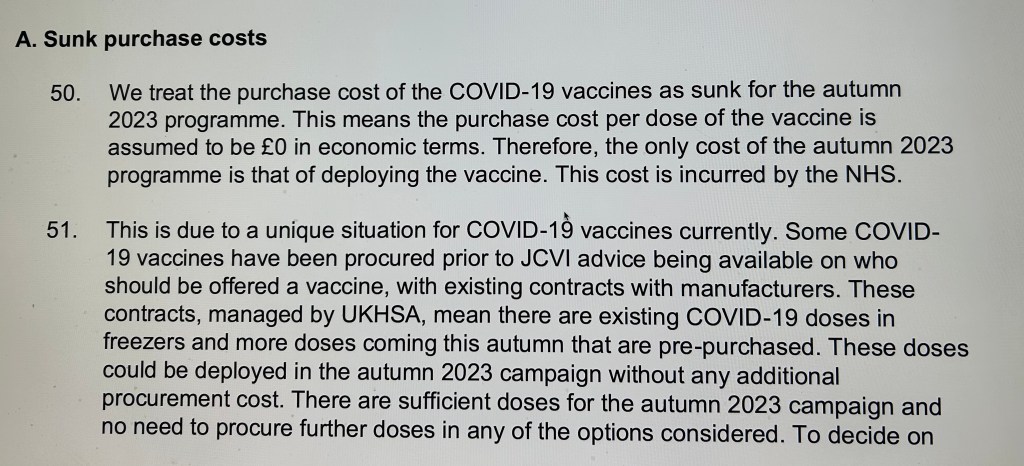
This essentially means that the government plans to throw away the vaccine purchased and treat it as a sunken cost – £0 in economic terms. To me or to any reader this appears odd, because the vaccine has already been paid for and could have economic benefits if administered. But it is one of the oddities of government economics.
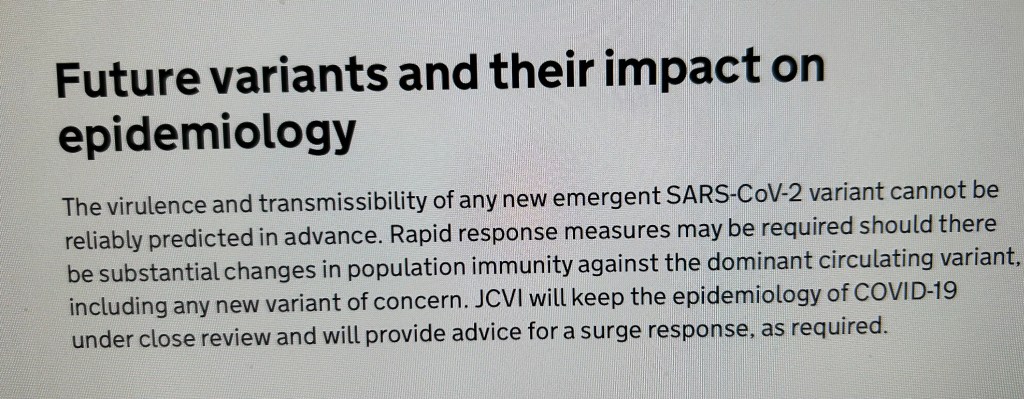
It is also outrageous in my view as the UK is experiencing a surge in infections at present. The only glimmer of hope is that the JCVI might change the advice at the last minute given there is scope in the guidance to respond to a surge response.
Details
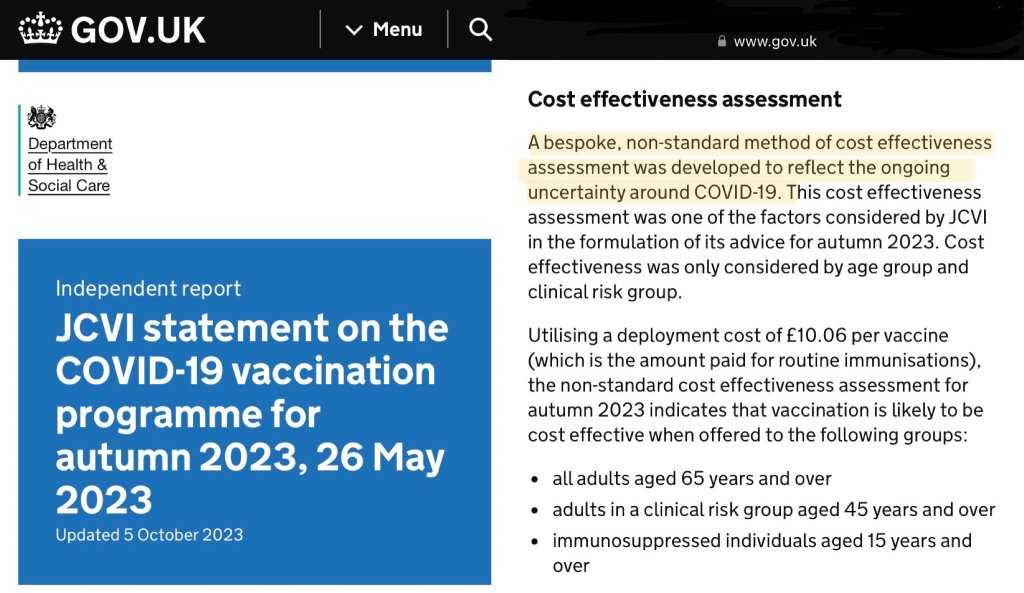
But where did this recommendation to restrict access to the vaccine come from? Again, we must be grateful to ‘Cat in the Hat’ for ploughing through the fine detail. Essentially the government is using something called ‘A bespoke, non-standard method of cost effectiveness assessment’ developed to reflect the ongoing uncertainty around Covid-19.
Sounds suspicious? Yes it is. Many areas of government policy making have uncertainty surrounding them, but most stick to the usual methodology.
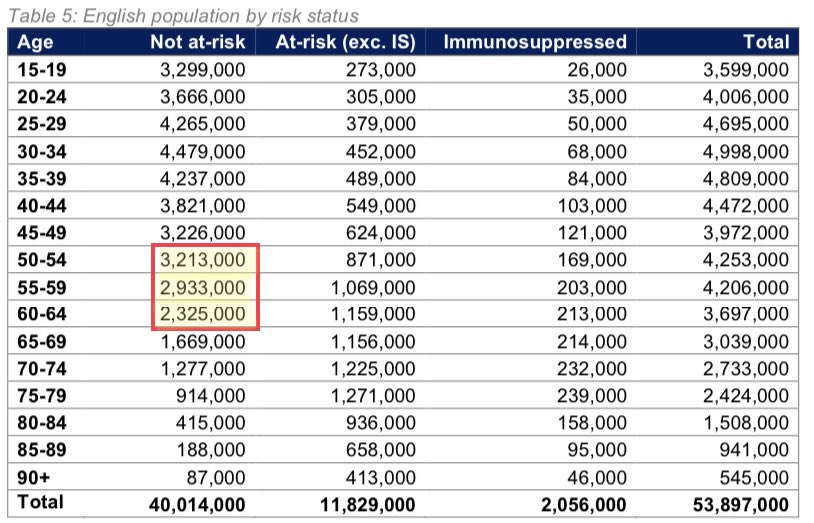
Due to this decision to reduce eligibility for the Autumn booster, there are now 8.5 million people aged between 50-64 years but not considered ‘at risk’ who have been unable to get a booster this Autumn despite the fact that vaccine doses have already been bought for them! And for those eligible people who received the ‘old vaccine’ in September before the new up to date vaccine was rolled out on 2 October, many will be distressed to learn that the ‘new’ vaccine will be sitting in fridges waiting to be thrown out.
Copied from Cat in the Hat
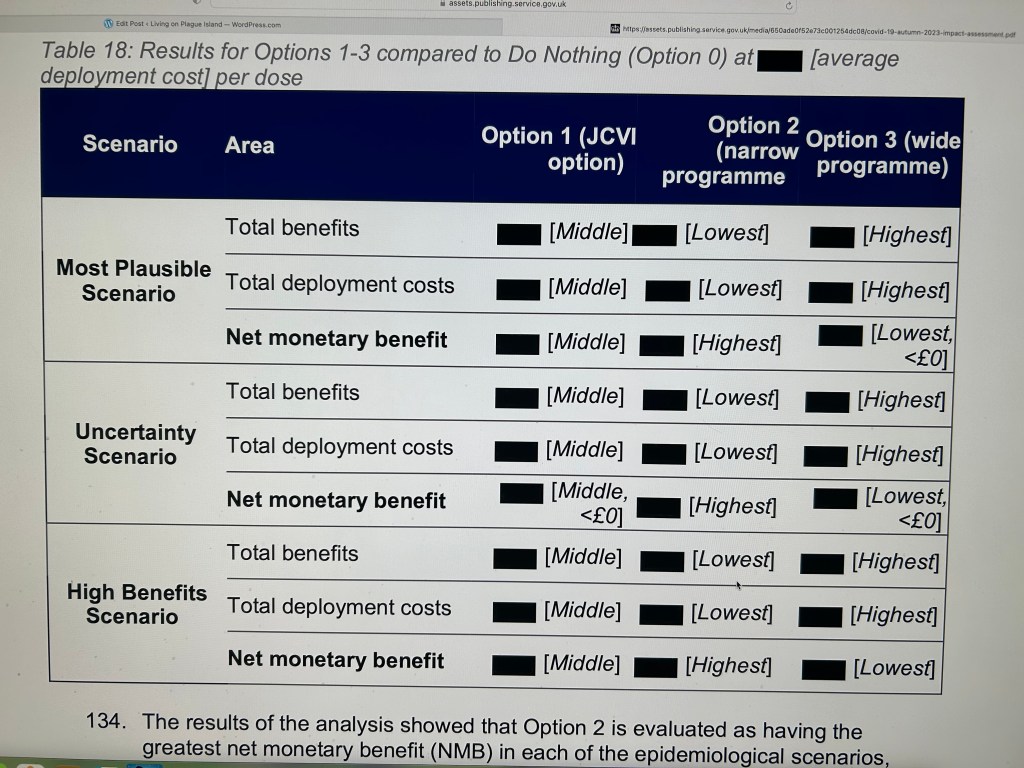
If it is any consolation it could have been worse (option 2)! Having received the advice of the JCVI the government looked in detail at three options, again based on the rather unusual cost-effectiveness methodology. The options were:
- Vaccinate all adults >65 plus all at risk or immunosuppressed
- Vaccine all adults >80, all at risk >45 plus all immunosuppressed >6 months
- All adults > 50 plus all at risk or immunosuppressed >6 months.
The government then calculated how many ward and ICU hospitalisations would be averted under each option and how many non hospitalised symptomatic infections would be averted. Again I am grateful to ‘Cat in the Hat’ for this analysis.
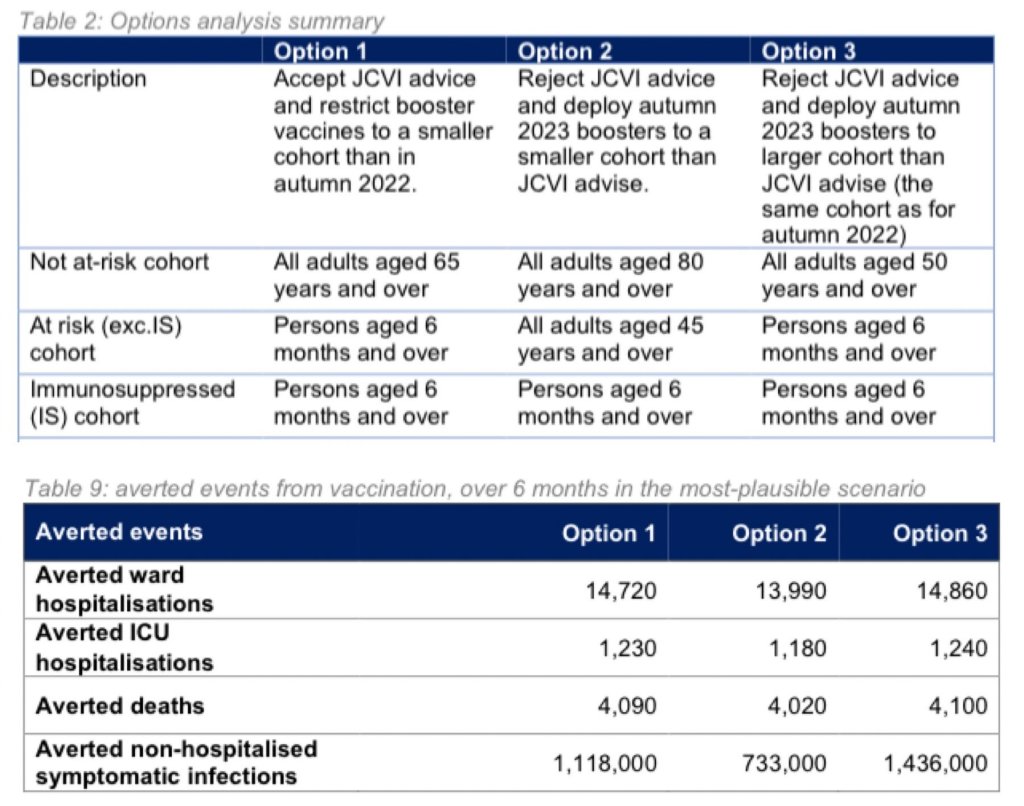
As we can see from the above table, going for option 3 rather than the chosen option 1 the government claims it would have averted an additional 140 ward hospitalisations, 10 ICU hospitalisations, 10 deaths and 318,000 non-hospitalised symptomatic infections.
The modelling that this is based on has been redacted and it’s impossible to verify these models as highlighted by Cat in the Hat, ‘but the hospitalisation figures in particular seem low given that Covid hospitalisations in the 18-64 year olds ran into tens of thousands last Winter.
As discussed by Cat in the Hat on twitter, the government then went on to attempt to attach monetary values to the various real life savings outlined in the above table, including:
- savings to the NHS,
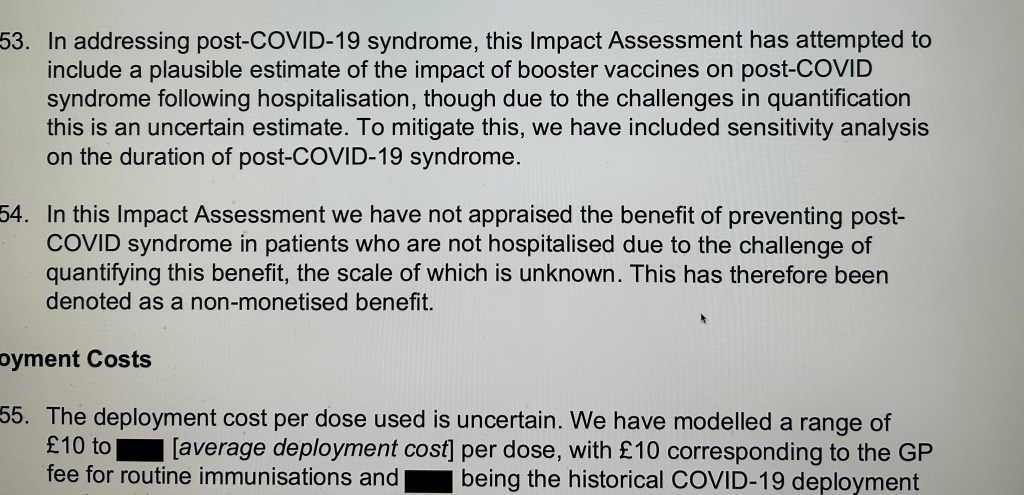
- an estimate of the savings in terms of Long Covid (assumptions and details redacted but buried in the detail it is clear that there are assumed to be no Long Covid costs endured by non hospitalised patients!), this is clearly wrong.
- indirect health benefits to the wider population, and non health benefits. How were these calculated? You guessed it – we are in the dark.
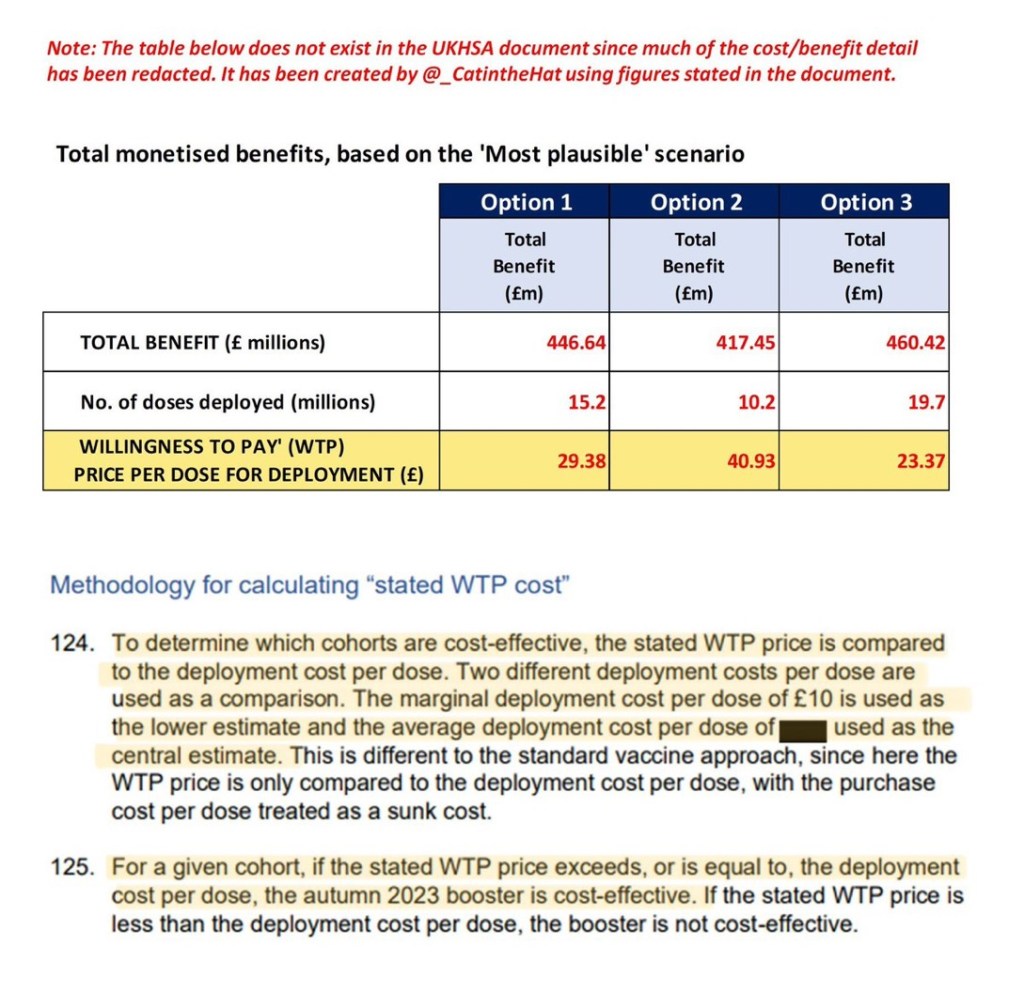
After a lengthy process the Cat in the Hat then summarises his/her total estimates of the monetary benefit that accrue from each of the three options. All three options have a monetary gain that is far greater than the marginal deployment cost per dose of £10 – the monetary benefit of option 3 which would see all >50’s vaccinated is estimated at £23.37 million.
However, Cat in the Hat has found a further sting in the tail which is outlined in the following copied section. Qaly’s stands for the ‘Quality-adjusted life year’ and is used in economic evaluation to assess the value of medical interventions.
Qaly’s are normally given a societal value of £70,000 in Cost Benefit Analysis but this is not the case with Qaly’s for vaccines. Cat in the Hat’s argument is that given the costs to society of continuing waves of Covid-19, the normal £70,000 figure should have been used.
This raises the cost effectiveness of all of the options considerably to :
Option 1 : £92.74 per dose
Option 2: £128.92 per dose
Option 3: £73.93 per dose.
Concluding Comments
Cat in the Hat has clearly done a fine job in uncovering this. In response to the thread on twitter he/her has given permission to use the material and it is likely that the North West Bylines will be publishing it, but it ought to be published more widely. I will include a link when this happens.
My assessment is that we must acknowledge that economic modelling in government is by its nature complex. However, I have never in my entire career seen such a high degree of opaqueness and redaction of data that modelling is based on.
I normally have some sympathy for those involved in modelling – it’s a difficult job and only a handful of people understand the detail.
However, a key weakness of modellers in general, in my opinion, is that they are unwilling to say when a task is far too difficult to carry out because there is a high level of uncertainty, a lack of detailed data and a general secrecy surrounding the data they need to use.
Rather than becoming mired in meaningless, opaque calculations, would it not have been better, in this case, to decide on vaccine policy in more transparent, common sense terms, possibly drawing on a wider range of data and surveys of the preferences of the NHS, the public and firms across the economy? Deliberative research involving the public either through on-line forums or focus groups would be ideally suited to this task.
Furthermore, despite all the secrecy it is still clear from the analysis presented above that vaccinating a bigger proportion of the population and even giving everyone the option of getting vaccinated as in North America would have been a good option. This is my view anyway.

Leave a reply to Lee McAulay Cancel reply