The long awaited Covid Inquiry report of the investigations into the healthcare systems (module 3) appeared on 19 March 2026 following on from ten weeks of public hearings held in the Autumn of 2024. This blog discusses the key findings and recommendations and outlines why this represents a major victory for the Clinically Vulnerable Families group.
Summary of Key Findings and Recommendations
This section covers four key issues: Did the NHS collapse? and how can we avoid this in future?; Infection Prevention and Control; Protecting Clinically Vulnerable people – particularly the Shielding Programme, and Long Covid. Anyone looking for a summary of the key messages and recommendations should listen to the introduction to the report given by chair, Baroness Hallett to coincide with publication – see the Inquiry YouTube channel. The full report can be found here.
Did the NHS collapse?
The overarching message is that despite various efforts to increase both physical space and staff capacity, the NHS came very close to complete collapse. The report notes that this largely reflected the fact that the UK went into the pandemic with an NHS under severe strain and operating near full capacity (para 5.113).
Baroness Hallett acknowledges that complete collapse across the system was only avoided by the extraordinary efforts of staff. It is however, important to draw a distinction between complete system collapse and the situation in individual settings at various points in the pandemic. In para 10.123 for example, the powerful witness Dr Kevin Fong describes the dire situation in one particular setting, concluding that ‘it is the closest I have ever seen a hospital to being in a state of operational collapse.’
The report makes it clear that not all patients – Covid-19 and non Covid-19 – received the level of care that they should have. Staff – patient ratios, including in Intensive Care Units (ICU’s) were diluted, shortages of medical equipment and oxygen were a big concern, not all patients seriously ill with Covid-19 were admitted to hospital or to ICU despite their poor condition, ambulance delays were common place, inappropriate do not attempt resuscitation orders were imposed unilaterally, and staff were left to make impossible decisions about who to admit to ICUs. Meanwhile non-Covid patients with life threatening conditions did not always receive timely treatment and important cancer screening programmes were paused. Was this collapse? See the following video from Baroness Hallett’s introduction.
More generally, the report notes that the ‘stay at home, protect the NHS‘ messaging generated a fear of catching Covid-19 in medical settings, and served to discourage people from seeking medical help when they needed it, sometimes with tragic consequences.
Summing up in the words of Baroness Hallett :
‘Ultimately, it is a question of whatever word is chosen, the impact of the pandemic on healthcare systems, their staff and their patients was devastating. We must never reach that point again. The recommendations set out in this Report are intended to minimise that risk.‘ (para10.124)
No doubt because of the constraints of her remit Baroness Hallett steers clear of making any recommendations on resourcing of the NHS more generally, but focuses on the need to be able to scale up. These two points are of course related as ability to scale up will depend on resources.
The recommendations relevant here include the following two on the need for planning to enable scaling up capacity when needed:
The report also recommends the need for a framework to be drawn up on allocating intensive care resources:(
For many people working in health and social care , the Covid-19 pandemic had a significant and long-lasting impact on their physical and mental health and wellbeing and exacerbated the stresses and strains of working in healthcare systems that lacked resilience. Despite this, many staff received little or no support and many staff has since left the NHS. Recommendation 10 seeks to address this.
Infection Prevention and Control?
As noted by Lara Wong below the inadequacies of the Infection Protection and Control guidance in place in 2020/21 had a significant adverse impact on infection rates and deaths.
Infection Prevention and Control guidance is of course critical to protecting both patients and staff and was the responsibility of the UK IPC cell set up in February 2020. The module 3 report describes it as ‘evolving informally ‘(para 1.32) and it was plain for all to see that there were major problems. It is important to mention here that across the years since 2020 CATA (Covid Airborne Transmission Alliance) have worked tirelessly to try to uncover what was actually going on against a barrage of silence and appalling delays in responding to FOI requests directed at the Department of Health and Social Care and elsewhere. CATA were a core participant in module 3 and have published their response to the report.
Time and time again the module 3 hearings witnessed what felt like a complete disconnect between independent scientists called to give evidence, Professor Clive Beggs for example, and government witnesses, including former members of the IPC cell. Throughout the hearings we heard how the IPC cell clung to the idea that Covid 19 was transmitted by contact and droplets, failing to question themselves critically about whether it might be transmitted via aerosols through the air . This narrow thinking was evident even when there was significant evidence to suggest they were wrong – for example in December 2020.
How Covid-19 was transmitting had fundamental implications for mitigation measures deployed. Ventilation and high quality PPE eg FFP3 masks, are key to protecting people against an airborne virus, yet because of flaws in the guidance these measures were not in place at the height of the pandemic . For example FFP3 masks were not deemed to be necessary for staff not involved in so called‘ aerosol generating procedures’ (mainly in ICUs).
This failure to protect both staff and patients had tragic consequences for both staff and patients.
Of course, there will always be debate and uncertainty early on in the life of any new novel virus about the route of transmission. It is therefore welcome that Baroness Hallett has accepted the argument for in future assuming that all plausible routes of transmission are possible until proven otherwise. Moreover, she goes on to accept the argument that the distinction between droplet and aerosol routes of transmission was somethingof a false dichotomy. This is key. Policy makers responsible for resourcing decisions will always want to assume the best case scenario eg in this case transmission via close contact which is easier to control. But had the UK assumed the worse ie. Airborne transmission from the start and implemented appropriate mitigation measures it would have saved many lives.
There has always been a suspicion that the IPC guidance was influenced by the shortage of PPE at the time. However, in commenting on the inconsistencies between the evidence given by different witnesses regarding whether the drafting of the IPC guidance was influenced by a general shortage of high quality PPE, Baroness Hallett concludes that ‘ practical considerations of supply should have been irrelevant to assessing the level of risk posed by specific routes of transmission ‘. (para 1.90).
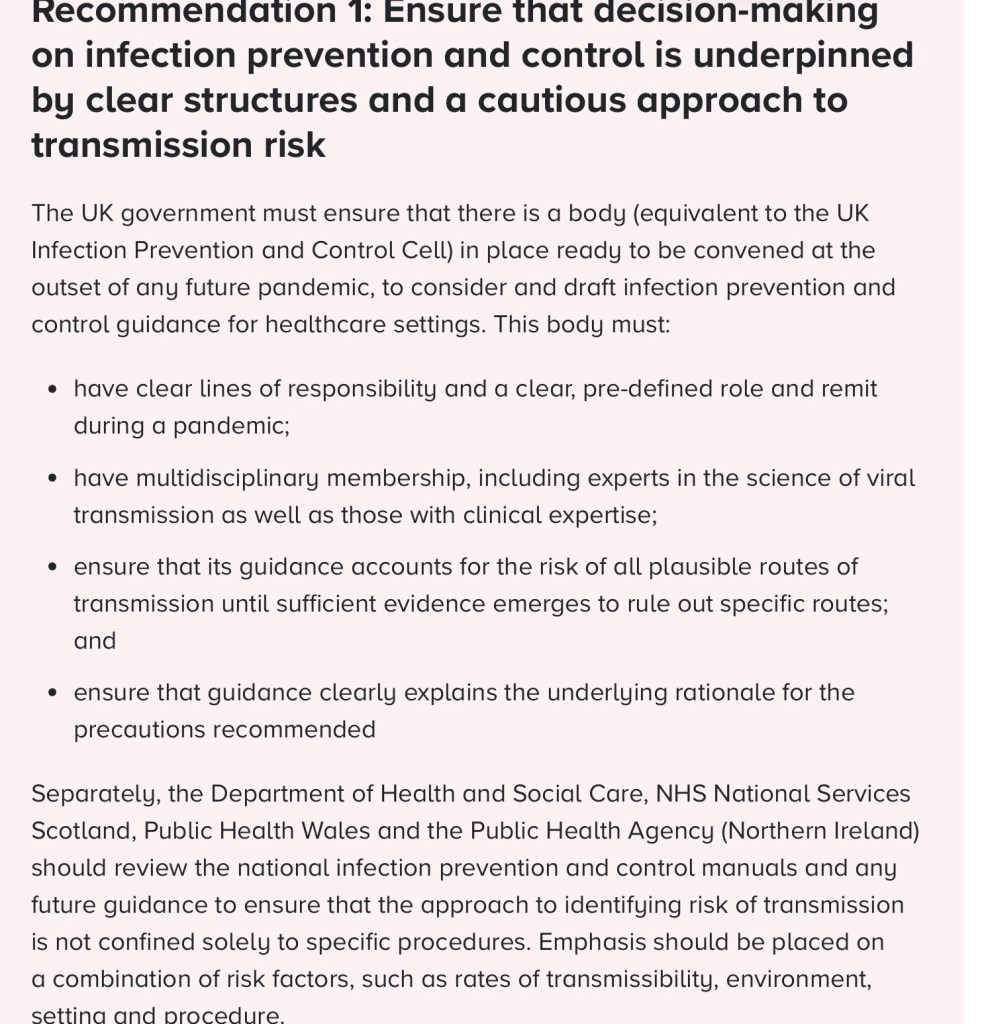
In addition to their initial assumptions (which they clung to for over a year after there was good evidence to suggest these were wrong ) it is also a relief that Baroness Hallett has accepted the argument that the way in which the IPC cell operated was flawed. It lacked formal governance, its remit was unclear and it relied on people with a very narrow range of expertise, and it failed to take account of what experts outside of the cell were saying.
Dr Shin, Dr Warne and Professor Gould set out one the key points in their evidence:
“At a time of national emergency where IPC can prevent, or fail to prevent, hundreds of thousands of hospital-acquired infections, interpretation of a rapidly changing evidence base must be as skilled, comprehensive, and unbiased as possible to ensure that guidance is of the highest possible quality. This requires a diverse and large team.”229 para 1.139
Lady Hallett goes on to recommend that the remit of the IPC needs to be clearer and that the membership of any such future body needs to be multi disciplinary and include experts in public health and viral transmission. This is captured in Recommendation 1 – see below.
As well as good quality PPE the other main weapon against airborne viruses which hang about in the air rather like cigarette smoke is of course good ventilation. Specifically on ventilation, the chair concludes that failing to recognize the importance of good ventilation, including via relatively cheap HEPA filters, in preventing the spread of Covid-19 ‘was likely due to the belief among members of the IPC cell that Covid 19 was not ordinarily spread by aerosols’ (para 1.99). )
It is encouraging that in para 1.105 she concludes that:
‘All hospitals built in England in the context of the UK government’s New Hospital Programme – and any new facilities built in Scotland, Wales and Northern Ireland – ought to be designed in a way that maximises the opportunities for effective ventilation. In the short term, the use of HEPA filters should be prioritised within healthcare across the UK’.
As noted by Lara Wong – see below, the Clinically Vulnerable Families group has been promoting the importance of HEPA filters for years, and many members like myself have been using them for years. The challenge is now to ensure this recommendation is acted upon in a context of low awareness of the function and benefits of HEPAs.
Shielding
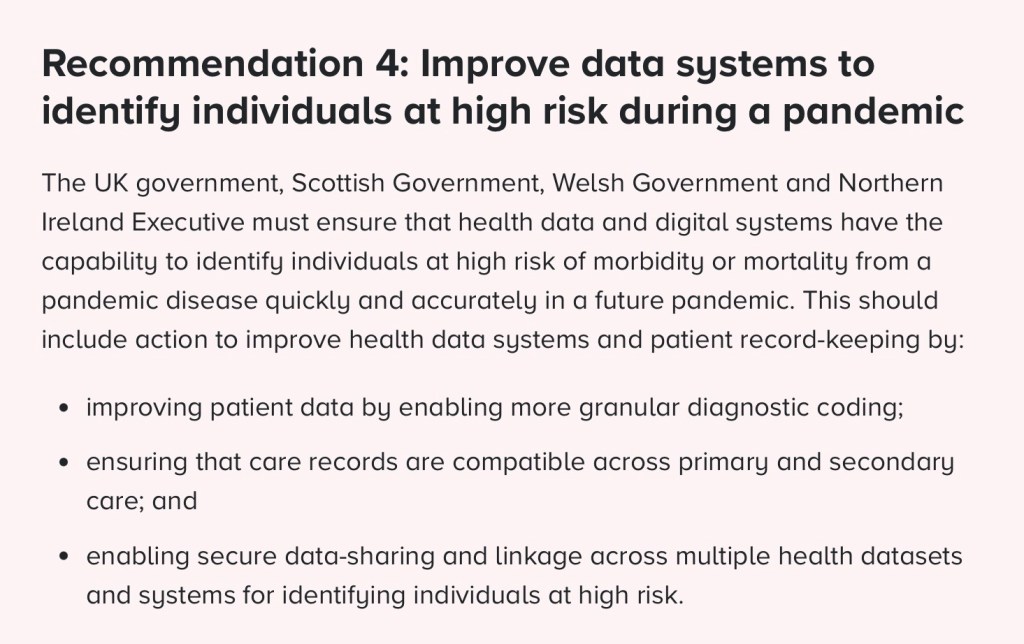
A formal shielding programme was put in place at the height of the pandemic fromMarch 2020 with the aim of trying to protect the most clinically extremely vulnerable individuals. However, it is clear that the process of deciding who should be shielding was flawed. This meant that not everyone asked to shield should have been, whereas some people who should have been shielding were not on the list. This largely reflects a lack of readily available data as NHS records were found to be not fit for purpose. See the following video clip from Baroness Hallett’s introduction.
Recommendation 4 attempts to address data problems.
The report also finds that shielding was associated with increased loneliness and isolation. The chair concludes that in future, the consequences of introducing a shielding programme need to be carefully considered alongside other considerations and this needs to be underpinned by better pre-pandemic planning.
More generally, Baroness Hallett appears to have accepted the point made by CVF that neither those shielding nor anyone else was provided with the kind of ‘empowering’ information they needed on how to keep themselves safe, including when attending medical appointments. And when shielding was ended abruptly CV people, many of whom continued to face serious risks, were given no information on how to keep themselves safe in a world where everyone appeared to be behaving as though things were back to normal . It is therefore encouraging that the report goes on to recommend improvements in communications – ‘that there should be consultation with people impacted by the shielding advice and representative groups to ensure that appropriate transitional advice and support is available.’
Long Covid
For many people post viral symptoms or Long Covid has had a devastating impact on their lives. Authorities were slow to recognise this.
It is acknowledged that there are difficulties in diagnosing long covid given that 200 plus different symptoms of the condition have been identified. And a lack of testing to identify definite Covid cases early in the pandemic and a general lack of awareness and knowledge of Long Covid within the primary care sector were also explanatory factors.
Nevertheless the UK response had/has many inadequacies. These include a lack of research funding, and a lack of adequate data on the prevalence of long covid. Provision for treating Long Covid has been patchy and the withdrawal of funding and resulting closure of many of the specialist ‘one stop shop’ centres that did exist has had serious consequences.
Looking to the future, Baroness Hallett concludes that better planning in is needed built on an assumption that long-term post-infection conditions are likely to increase significantly from the very earliest stages of the next pandemic disease. She concludes –
‘ the best way to limit the number of people who suffer post-viral conditions is obviously to limit the number of people who get infected. However, governments must plan on the basis that ….many people will be infected and many will suffer long-term. None of the four nations currently has a plan in place to respond rapidly to the long-term health consequences resulting from a future pandemic disease.179 UK healthcare systems must be equipped to deliver care for patients affected by long-term illnesses resulting from a future pandemic disease and play their role in improving understanding about such illnesses and the effectiveness of interventions. This requires the timely collection and analysis of reliable data, research into the impact of long-term illnesses and the evaluation of treatments as they develop’.para 8.75
She goes on to conclude that
‘long covid clinics which provide a one stop shop’ based on holistic treatment from a multidisciplinary team are ‘both clinically effective and cost -effective’ and she recommends ‘ this model of care.’
And that:
‘Healthcare systems must be supported and prepared to meet the increased demand for care and treatment that will inevitably occur when large numbers of people are affected by post-infection conditions, not just during the peak of a pandemic, but for years to come, and potentially the rest of their lives.‘
Report is a Victory for Clinically Vulnerable Families
After hours locked in with the report, along with the other core participants, Lara Wong, head of CVF was the first to emerge to into the crisp Spring sunshine after the report was published at 12 noon on 19 March. The waiting press witnessed Lara’s welcoming comments – see a video via YouTube. Lara’s subsequent blog expands on why this should be regarded as a victory. Here are some key paragraphs from Lara’s blog.
✓ THE SCIENCE ON AIRBORNE TRANSMISSION: CONFIRMED
‘From our very first submissions, Clinically Vulnerable Families argued that there was a fundamental misunderstanding at the heart of infection control policy… was driving the wrong decisions and leaving people at the highest risk unprotected…
The report identifies three fundamental flaws in the UK’s infection prevention and control approach. The guidance, Baroness Hallett finds, was:
“wedded to an outdated and scientifically inaccurate understanding of how the virus spread” Module 3 Report
The consequences were exactly what CVF said they would be: airborne protections were deprioritised, ventilation was neglected., and people at the highest risk were left unsafe in NHS settings. …. The science was on their side the whole time. The Inquiry has now confirmed it.‘
✓ CLEAN AIR IN THE NHS: NOW A RECOMMENDATION
‘The report recommends that HEPA air filtration be prioritised across NHS healthcare settings in the short term, and that all new NHS facilities be built with effective ventilation. The Inquiry’s own expert, Professor Beggs, described HEPA filters as ‘cheap’, easy to install, and doing ‘a similar job to ventilation.’ We (cvf) had brought them to the hearing centre before any expert said this. We had measured the air quality. We showed Baroness Hallett the numbers.‘
‘Now the NHS must do the same. When hospitals are safe enough for the most vulnerable, they are safe enough for everyone. I will be watching – and asking, loudly and specifically – how and when this recommendation will be implemented. A recommendation without a timetable risks all too easily being shelved.‘
✓ THE RIGHT TO WEAR A MASK: VINDICATED
‘Every Clinically Vulnerable Families member who was asked at a hospital entrance to remove their FFP3 and replace it with a surgical mask – told that their own evidence-based protection was less appropriate than a poorly fitting surgical one – has been vindicated today. The Inquiry’s expert witness, Dr Ben Warne, stated it plainly, and Baroness Hallett quoted him with approval:
“There was no good reason to prevent patients from wearing face masks.” Dr Ben Warne, IPC Expert Witness
The report also records that when routine masking guidance was relaxed in May and June 2022, the proportion of CVF members delaying or cancelling NHS appointments rose sharply.…
High-grade masks are not a political statement. They are protective devices that make healthcare accessible for people who cannot afford to catch an infection. They should never have been taken from us. The Inquiry has said so. Next, we need enforceable guidance to back us up.‘
✓ EMPOWERING PEOPLE AT HIGH RISK: A COMMITMENT FOR THE FUTURE
‘The report states that advising people at high risk on how to protect themselves will be:
“vital in any future pandemic”
During the height of the pandemic, our members were not given information about appropriate airborne protections. They were given a letter telling them to stay home – and then, when shielding ended, nothing. No guidance on assessing and managing personal risk. No framework for re-emerging into a world that had decided that ‘Covid was over’. Some of our members have never fully re-emerged. The Inquiry has recognised this as a failure. That recognition matters.‘
◉ DNACPRS: ON THE RECORD – AND NOT YET RESOLVED
‘The report confirms what Clinically Vulnerable Families submitted: that ‘Do Not Attempt Cardiopulmonary Resuscitation’ notices were placed on patients’ records without their knowledge or consent, based on underlying conditions rather than individual clinical assessment.…The Care Quality Commission found ‘a worrying picture of poor involvement, poor record-keeping, and a lack of oversight.’ All confirmed.‘
Implementation
As discussed previously – (see my previous blog), the key challenge will be to ensure the findings and recommendations from the Inquiry are implemented. On this Baroness Hallett makes it clear that her recommendations should be implemented immediately. See the following clip
The issues raised in the report remain pertinent today, especially for clinically vulnerable families many of whom remain fearful of attending healthcare settings due to inadequate infection control measures and lack of clean air. It is therefore inappropriate to sit on the findings in typical civil service and political fashion – we need implementation to happen now.
Moreover, as Hallett reminds us, it is not if, but when the next pandemic strikes. The resilience of the healthcare systems and appropriate IPC measures underpinned by accurate scientific evidence will be key to doing better next time.
Speaking to Channel 4 Sarah Steven of CVF makes the point that if we don’t start to make changes now clinically vulnerable families will simply become the bereaved families.
In this context it is worrying that many commentators think we are in a worse position now than in 2020 and this makes the task even more urgent. Although there may have been some recent improvements, it remains the case that ambulance delays, lack of timely access to primary care, and corridor care in hospitals are all to familiar in 2026. See, for example, the following video of Nicola Ranger of the Royal College of Nursing responding to the report:
In a recent piece, Professor Christina Pagel also reminds us just how badly the UK performed, particularly in wave two when the scale of deaths and pressures on the system reflected a complete failure to take the necessary preparatory actions in the second half of 2020.
Christina ends on a moral note – it would be disrespectful to all those who held the system together and those who died not to implement the findings from this inquiry:
The world has moved on, plunged into crisis after crisis and there seems to be a collective determination to forget and never speak of the pandemic. But to ignore the findings of the Inquiry – to refuse to learn from the evidence and the pain – disrespects the sacrifices of those who held key services together and those who died. It would devalue all of us – and leave us as unprepared for the next pandemic as we were for this one.(C Pagel 2026)
Next Steps
There are of course seven module reports still to be published and the final report of the Inquiry will not be published before next year – for information on the timetable see my previous blog. It is expected that the remaining module reports will have common threads running through them with appropriate cross referencing. It is important that one of the key messages should be the need for better guidance on IPC measures – good ventilation and high quality PPE across the issues looked at – for example in vaccination centres, care homes, education settings, public buildings and leisure centres. This would be good for the economy as well as the wellbeing and health of everyone.
In my assessment the current module 3 report could have been more forceful about the differences in quality between different types of ‘masks’. However, we should remain hopeful that the final report will make it crystal clear that ill fitting surgical masks (baggy blues) were never adequate and cannot protect people from an airborne virus. See the following video clip from an excellent lecture delivered by Nancy Malek.
Also under the heading of outstanding items – this report does not recommend legal recognition of clinical vulnerability as a protected characteristic. However, as Lara Wong notes in the blog referenced above, Module 3 was our first module, and our legal rights argument took time to develop throughout the inquiry via testimony and other evidence.
Lara concludes that:
‘by the time we reached Module 10 – the Inquiry’s final investigation into the impact of the pandemic on society – our argument was more fully formed. The Equality Act does not protect many people with serious underlying health conditions, who face increased health risks. They fall through the gaps in the law and the pandemic exposed this catastrophically. As a consequence their protections were switched on and switched off at the discretion of officials, with no specific recognition or rights to fall back on.‘
The argument is still not finished. Final written submissions are yet to be completed. The next pandemic will come. There are millions of people with conditions like cancer, neurological diseases, asthma, diabetes, heart disease, and weakened immune systems who deserve to have their safety guaranteed in law – ‘not temporarily extended or withdrawn depending on the whim of the government‘.
Gillian Smith
7 April 2026

Leave a comment