
The public hearings of the tenth and final module of the UK Covid Inquiry ran from mid February for three weeks. In the video embedded here Ben Connah, Secretary to the Inquiry, explains the scope of this stage on the impacts of the pandemic on society.
This is a very wide ranging module which picks up on issues in danger of falling through the cracks of other modules. The module involved no fewer than thirteen core participants, including voluntary groups such as MIND, the Domestic Abuse group as well as the Disabled People Organisation, and the Clinically Vulnerable Families Group. Groups representing the bereaved were also strongly represented and were provided with their chance to explain the devastating impact that the pandemic continues to have on the lives and well-being of those left behind.
This short blog picks up on some of the key issues to emerge from the hearings. I don’t attempt to cover all of issues and evidence presented and focus, in the main on the interests of the Clinically Vulnerable Families Group.
Bereavement
This stage of the Inquiry heard more than eight hours of harrowing evidence from witnesses who had been bereaved by the pandemic. They spoke about the traumas of losing someone in completely unexpected circumstances and it is clear that many people have never been able to come to terms with the deaths of loved ones. This lack of closure often reflected the consequences of the rules in place at the time, including the restrictions on visiting dying patients in hospitals and care homes, coupled with intense fears about how loved ones died. Lack of access to bodies (very important in some cultures) , and funeral arrangements with restricted numbers and social distancing also served to heighten the sense of grief. Some witnesses spoke about how customs appropriate to their cultures, including the holding of wakes, were not allowed. It is also clear that the issues surrounding ‘partygate ‘ and the fact that many of those in power failed to follow their own guidance served to intensify the anger and sense of loss and injustice felt by many bereaved families who had followed the guidance and suffered greatly as a result.
For many families their distress reflects the fact that many of the deaths are regarded as having been unnecessary but were caused by political decisions such as the UK going into lockdown too late, and then failing to learn the lessons of wave 1 which would have lessened the devastating consequences of wave 2 in late 2020/early 2021. And for others who lost someone because they caught the virus in a healthcare setting, the knowledge that key lessons about Infection, Prevention and Control were ignored again only serves to intensify their sense of loss.
Inequalities
People were not impacted equally by the pandemic and this was a key theme running throughout the hearings for this module . Deprived social groups, people living in deprived areas, black and minority ethnic groups, people living with disabilities and clinically vulnerable people and their families were hit disproportionately and suffered a range of physical and mental health and other impacts, including death.
Socio Economic Inequalities
The Inquiry heard extensive evidence from Professors Marmot and Bambra, and others, on how the pandemic served to widen social and economic inequalities and deepen poverty experienced by a significant proportion of the population.
Food poverty jumped to new levels during the pandemic as did housing pressures, and the percentage of household income spent on rent increased during this period.
It is clear that overcrowded accommodation made it difficult for households to limit the spread of the virus. As explained by Prof Laia Bécares, multigenerational households which were far more likely to be overcrowded, often contained frontline key workers and children in schools as well as a disproportionate number of people over 65 with clinical vulnerabilities. It is not difficult to see how the virus could easily spread in these households with devastating consequences. And given that some black and minority ethnic (BME) groups are far more likely to live in these circumstances it also constitutes part of the explanation for the disproportionate number of Covid-19 deaths experienced by BME groups.
The type of jobs done by workers was also a key explanation for differential exposure to the virus especially in the absence of adequate PPE and ventilation. Those called upon to perform front line roles in order to keep society functioning- including those working in supermarkets and food production, for example, were placed in greater danger than office workers who could work from home.
The result was large inequalities in mortality rates between deprived and non deprived areas as revealed in the following chart contained in Marmot and Bambra’s written statement . We can see how in 2020 and 2021 the most deprived fifth of areas (1) experienced far more Covid-19 deaths than other quintiles.
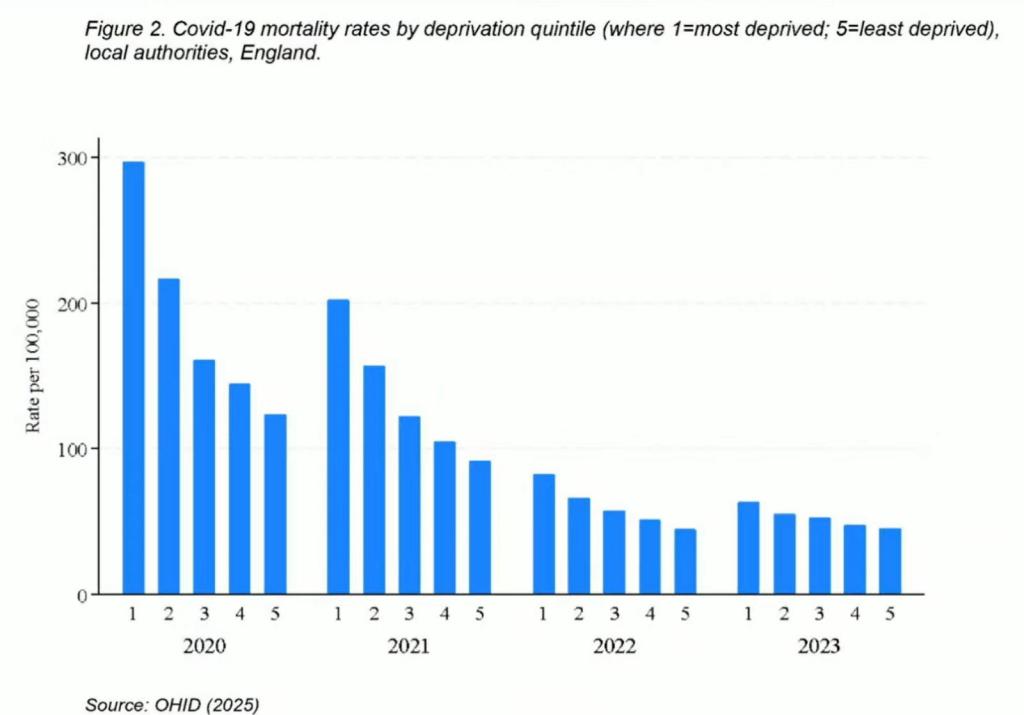
In terms of planning for future pandemics the key message from Professor Marmot is that if the existing levels of inequalities are allowed to continue it is inevitable that there will be a high number of deaths from any future pandemic.
Mental Health
There is a complex interaction between physical and mental health. In his evidence Professor David Osborne highlighted that people with severe mental health problems were also more likely to suffer physical comorbidities and clinical vulnerabilities .
Moreover, such people were far less likely to seek help for their problems at the height of the pandemic because of the measures in place, shielding and general messaging around ‘stay at home – protect the NHS’. This point was picked up by a number of witnesses in addition to Osborne. Not only were people with pre existing serious mental health conditions less likely to come forward for treatment, in some, if not many cases, face to face services were not there in part because mental health staff had been redeployed to work on the Covid-19 front line in the context of a an overwhelmed NHS struggling to cope with the influx of Covid cases.
In addition to failing to cope with people with existing serious mental health conditions, the pandemic generated a blizzard of new cases reflecting the huge disruption to routine, loss of income, bereavements endured under tragic circumstances, physical illness, clinical vulnerability and family pressures experienced at the height of the pandemic. A number of witnesses told the Inquiry that statutory services were not in place during this period to deal with existing cases let alone new cases, and where services were available they tended to be online. Mental health charity MIND and others told the inquiry that the voluntary and charity sector was left to pick up the uptick in demand for support as best they could.
Moreover, the MH problems, particularly for clinically vulnerable families, did not end on ‘freedom day’ (July 2021). As explained in the Clinically Vulnerable Families (CVF’s) impact report discussed below, many people reported worsening mental health post the initial opening up in 2020 and also in 2021. Essentially, whereas they often felt at least partly protected during lockdowns, the opening up of society on the grounds that the NHS was no longer overwhelmed did not change their situation – they were still as vulnerable to adverse outcomes if they caught Covid-19. The problems were compounded because many people in the rest of society were behaving as though the risks were no longer present and on occasions directed abuse at those still taking care.
The impacts of the vaccination roll out sometimes tended to reinforce these problems because many clinically and (clinically extremely vulnerable (CEV) people could not take the vaccines for safety reasons or even if they could, did not receive the same protection from severe illness as the majority of the population. My blog on module 4 of the inquiry documents how the therapeutics programme was the poor relation to the vaccination programme and served to leave many clinically vulnerable people as exposed to harm as they were in 2020. The difference was they had to exist in a world that was increasingly aggressive to people who continued out of necessity to practice Covid precautions such as mask wearing and behavioural measures.
This situation also meant many CVF members were reluctant to return to unsafe workplaces particularly in situation when previous working from home (WFH) arrangements were coming to an end due to a ‘presentism’ mindset amongst some employers. In many cases this had disastrous consequences for the mental health and financial situation of clinically vulnerable people and their families.
People with Disabilities
This is a heterogeneous group consisting of people with both physical and mental disabilities. Some people with disabilities will also be clinically vulnerable, but this is a long way from always being the case. Similarly, not all clinically vulnerable people are disabled. This is why it is important not to assume that disability and clinical vulnerability are one and the same thing.
What is clear is that disabled people suffered disproportionate harm from the pandemic. They were significantly more likely to be living in poverty and in poor and overcrowded housing at the start of the pandemic and the gap between disabled people and the rest of society widened during the pandemic. Disabled people were also more likely to suffer domestic abuse during lock down and the withdrawal of normal face to face care services had a devastating impact on many people who rely heavily on health and social care services.
It is also clear that disabled people were often refused care if they caught Covid due to the use of ‘frailty scores’ and other measures in place to prioritise who, and who did not receive treatment. Inappropriate use of do not attempt resuscitation orders was also rife with the consequence that disabled people were left to die without any interventions, including oxygen.
In their final submission representatives of the Disabled Peoples Organizations echoed the key messages from Professor Marmott, that if we fail to address the deep inequalities in society, we will see the same deep inequalities in outcomes, including for disabled people, when the next pandemic strikes.
Clinically vulnerable families
There is a great deal of confusion about the use of the terms CEV (clinically extremely vulnerable), CV (clinically vulnerable) and immunosuppressed and immunocompromised. The distinctions between these various categories is often meaningless and a priority action should be to sort out definitions – essential if more meaningful data is to be gathered to inform policies in the future. In the rest of this blog we use the term clinically vulnerable (CV) people to capture all of these groupings.
On the eve of her third appearance before the Inquiry, Lara Wong, of Clinically Vulnerable Families (CVF)published an Impact on Society survey based on responses from 125 CVF members. This evidence, in conjunction with Lara’s witness statement, was used by the Counsel to the Inquiry in framing their questions. The Key findings included:
- Mental Health and Wellbeing – Many clinically vulnerable people felt isolation when shielding, and very stressed about their heightened risk of infection. For many respondents ongoing levels of depression and stress increased as society began to open up and they did not benefit from it. For many people the advantages afforded by vaccination did not apply to them and this sometimes led to a sense that their lives were not valued.
- Access to safe healthcare – the vast majority of respondents to our survey frequently described being forced to choose between whether to go ahead with treatment or consultation around their personal health issues and their need to keep safe and not catch the virus. The withdrawal of measures such as universal masking and short-term improvements to ventilation in healthcare resulted in cancellations and delays to medical appointments sometimes with adverse health impacts for CV people and their families.
- Social Care and Caring arrangements – respondents reported substantial disruption to in-home care, respite, and other social support, which was often withdrawn abruptly without replacement or clear communication. This resulted in huge pressures on unpaid carers.
- Work, Key Workers and Finances – respondents often indicated that they felt unsafe returning to work and were often refused reasonable adjustments. This was particularly true of household members of a CV person but often also applied to clinically and CEV people themselves. Lack of safety of workplaces sometimes caused a complete withdrawal from the labour market and significant loss of income. The following quote from an actress illustrates how much many people lost due to being clinically (extremely) vulnerable – ‘the door to every aspect of public life now appeared firmly locked’.
- Society, Culture and Hospitality – For many CV families, reopening was not experienced as freedom. The removal of protections such as masking, ventilation, occupancy limits made everyday activities more unsafe. Hospitality, retail, and tourism are repeatedly identified as especially inaccessible by respondents, and the government’s “Eat Out to Help Out” scheme amplified the divide by promoting indoor dining withouts safeguards at a time when no vaccines or treatments were widely available.
- Faith, Worship and Rites of Passage – Among respondents who had previously engaged in religious life, participation was widely affected. Early on in the pandemic online services, for example via zoom, helped, but later withdrawal of both mitigations and online access left many feeling abandoned or excluded from communities and key rituals.
- Housing and Living Situations – Many respondents explained that their housing situation made shielding impractical. This was especially true in overcrowded homes, some with shared bathrooms/kitchens, or limited ventilation and private outdoor space as discussed above.
The key points from Lara Wong’s evidence are captured in the following thread of video clips.
Lara emphasised the multi layered nature of impacts experienced by clinically vulnerable families. Despite this CV people were and are to this day often left to manage their own risks particularly in non lockdown periods, with little or no information being provided by government bodies on how to actually do this given the virus was/is airborne and it is difficult to control air quality through individual actions. Nor was there any serious attempt to inform the rest of population that there were groups of people that needed to continue to take care.
The consequence was that little or no attention was paid to the continuing needs of clinically vulnerable (CV) people when society did start to open up, and many CV people felt an increasing sense of isolation. Many lost friends and family who did not understand their continuing needs. Other people were on occasion abusive as a result, almost blaming CV people for the pandemic even though they were at the highest risk from it. And continuing caution in behaviours was sometimes perceived to be a mental health (MH) issue at root, rather than a rational response to continuing risks faced/face.
The multilayered nature of the issues is well illustrated by the fact that a number of vulnerable groups in society were also more likely to be clinically vulnerable including homeless people, prisioners and people suffering from domestic abuse – sometimes linked with being disabled. All of these groups were largely ignored by policy makers and the messaging at different stages of the pandemic was seen as unhelpful. For example, the stay home – protect the NHS message, combined with a lack of awareness of how to protect themselves against an airborne virus, may have discouraged victims of domestic abuse from attempting to escape from their situation.
In Clinically Vulnerable Families (CVF ‘s) closing statement Adam Wagner KC returns to these issues focusing on the key themes of safety, support and status – see this thread.
Under the Safety theme Adam stresses the importance of clean air and the structural challenges which need to be addressed now. He reminded the Inquiry of the need for CV people to have the right to participate fully in public and cultural life on fair and equal terms. In the absence of clean air CV people and their families have been left to make impossible risk calculations to inform decisions about whether to attend healthcare or work settings, for example. This message was strongly reinforced by the TUC representatives who identified an urgent need for change .
Under the Support theme Adam repeated the point that CV people received little or no support particularly when society began to open up. People were not given the skills and resources to be able to navigate new situations and take ‘personal responsibility in protecting themselves against an airborne virus.
Finally CV people need Status. The current position in which CV people are not recognised as an equality group needs to change given that there will always be a core group of people who are at high risk from infection. CVF are therefore calling for changes in Equalities Legislation to provide us with rights and status and also be provide a basis for regular data collection. Before the pandemic CV people existed but were invisible. The key message is that this must never happen again – we need to have a voice at the table when decisions are being made .
CVF Aims and Proposals widely supported
Throughout this module it was notable how many of the other core participants reinforced key CVF messaging particularly on the need for good ventilation and, where appropriate, PPE as a means of enabling safe access to healthcare, schools and colleges, public buildings, workplaces and cultural/entertainment venues.
There also seems to be an increasing recognition that this is not simply about planning for some future pandemic but it is about the here and now. Clinically vulnerable people continue to die from Covid and other infections, including those acquired in hospitals, healthcare, education and workplaces. Action is needed now.
Several of the bereaved people giving evidence to the inquiry picked up the point that it would have been possible for them to visit their loved ones in hospitals and care homes and have appropriate funerals had ventilation and access to good quality PPE had been better. And this would have helped alleviate the extreme anguish, stress and lack of closure suffered by tens of thousands of bereaved families. See the following clip from Rivka Gottlieb for example which acknowledges the point about the need to improve safety and change attitudes in the here and now. She calls for wider access to vaccination, legislation around air quality and mask wearing in healthcare settings. These things are not difficult yet would make a huge difference. She goes on ‘but we have allowed them to become politicised’.
And Sam Smith Higgins of the CBFJ Cymru made a strong plea to monitor air quality in order to endeavour to make hospitals safer – see video below.
Concluding Comments
This has been a wide ranging module that has thrown light on new issues, as well as going over old ground from a different perspective.
It is clear that the pandemic did not impact on everyone to an equal extent. Some groups in society bore the brunt including key workers who exposed themselves to the virus on a daily basis; those already socially and economically disadvantaged; disabled people and clinically vulnerable people and their families.
To avoid these disparities in future , policy makers need to be alive to the needs of real people, including disadvantaged groups in society. This reinforces the point made before that policy makers need to consult with a wider group of organisations and with a wider range of scientists – including public health experts and social scientists – to inform the design and roll out of policies. In other words policies need to be designed, implemented and communicated to reflect how real people live their lives and the challenges they face. This needs to include support for CV people and their families in navigating the dangers they face. I would also endorse the point made by Sir Michel Marmot, that it is not possible to avoid a high number of deaths amongst the most disadvantaged in society if existing levels of inequality are allowed to persist.
Finally it is clear to me that never again must science about how any new virus spreads become so confused and one suspects adjusted to suit political objectives and presentation . We now need honesty and public information about how Covid-19 and other airborne viruses spread and appropriate policy measures need to be rolled out in a timely way . We need safe air to be a fundamental right – something that could be achieved by better ventilation/air filtration and we also need an acceptance of mask wearing where appropriate in order to protect CV individuals, in fact we need to have a legal right to wear a mask . Remember, if it is safe for CV people it is safe for all.
Everyone, including politicians, must work to start to undo the damage of the last four -five years in which issues around safety from airborne viruses, including mask wearing have become politicised.
The module 3 report on Healthcare is due to be published later this week and will provide a clear indication of the chair’s thinking on airborne transmission, PPE and ventilation. Fingers crossed that Baroness Hallett will have carefully weighed up the evidence and concluded that the UK was slow to accept and implement the science that could have saved many lives. The tone should not be about blaming individuals, but about moving forward and improving safety.
At this point is worth repeating the key CVF messaging about Safety, Support and Status – please see the following video.
Gillian Smith
17 March 2026

Leave a comment