Earlier in the summer the government approved the Joint Committee on Vaccines and Immunisation (JCVI) proposals for this Autumn’s Covid-19 booster programme which were published last November as discussed in a previous blog post. This is despite all of our lobbying about the wrongheadedness of the proposals and the inherent dangers of further narrowing access to Covid vaccines. To try to stop some of this at this 11th hour the Clinically Vulnerable Families group needs your help. Please sign this petition , launched on 27 August 2025 which calls on the government to fund NHS COVID boosters for Clinically Vulnerable people, including previously shielded as CEV (clinically extremely vulnerable) people.
Details of Proposals
In sum the plans will lead to severe restrictions on who can get a free Covid booster this Autumn – over 12 million people are forecast to miss out. Only three groups of people will be eligible:
- people over the age of 75;
- individuals who are currently immunosuppressed under a very tight definition set out in the green book; and
- residents of care homes for the elderly.
The following groups who were previously eligible in 2024 for an Autumn boost will miss out:
- NHS staff and care workers, including informal carers;
- People over the age of 65 but under 75;
- People with underlying medical conditions who are not currently immunosuppressed enough to qualify – this includes almost everyone previously classified as clinically vulnerable and many people in the clinically extremely vulnerable group. It includes people with underlying heart and lung conditions, the clinically obese; people with severe diabetes, people with cancer to name a few;
- pregnant women.
This has all created quite a storm on social media but has largely been ignored by the national media no doubt in part due to the fact that the government announcement came out on 26 June at exactly the same time as the recent climb down on entitlement to personal independence payments and other benefits.
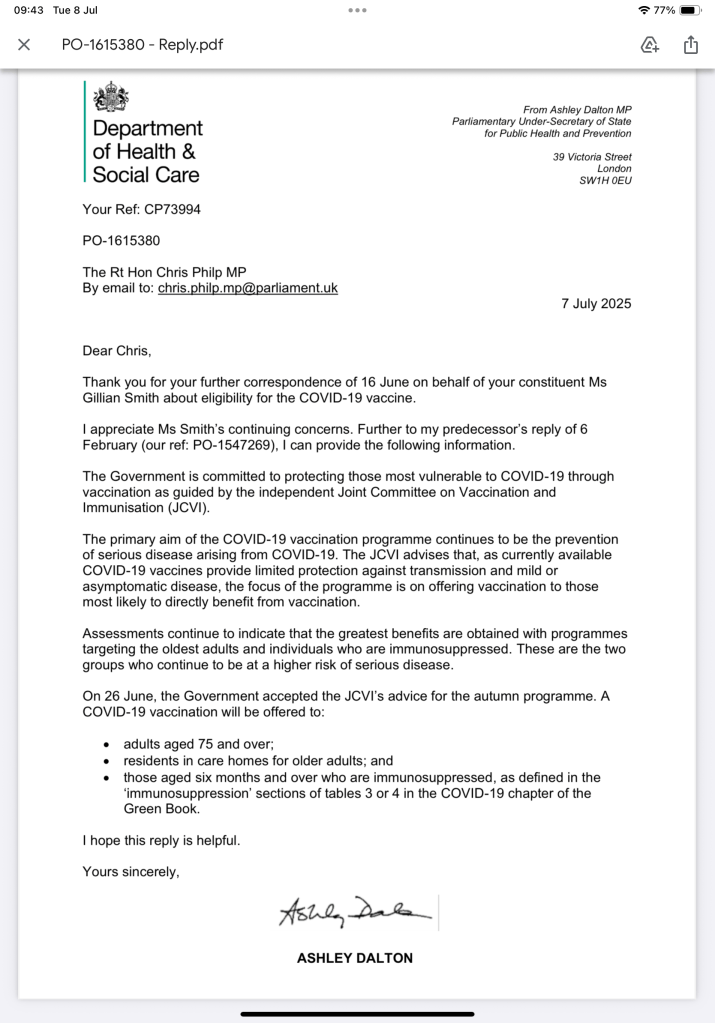
The rest of this blog summarises what is wrong with this approach, but first, an apology. As regular readers will know, I have been lobbying my MP who happens to be the shadow Home Secretary. On 16 June he wrote to the Department of Health again on my behalf and I fear this may have triggered this decision by government after seven months spent sitting on the JCVI recommendations – sorry!

I received the following reply on 7 July along with a cover note from my MP which made disparaging comments about the Labour Party.
Why are these proposals flawed?
The problems with the proposals, and the key arguments for extending entitlement to the Autumn 2025 Covid-19 booster programme to at least align with arrangements in place in Autumn 2024, include the following – for details see my previous blog post.
Lack of transparency
As usual the details underpinning the JCVI proposals are missing – we don’t know what data they have used and we have not seen their calculations.
Significant threat to health
The JCVI ignores the evidence that Covid-19 remains a significant threat to the health of people, including those with severe respiratory diseases, autoimmune disorders, cardiovascular conditions, and other chronic health issues. Most of these groups will be denied an Autumn (or indeed any) boost against Covid-19.
The JCVI proposals which have been accepted by the government, are based solely on their modelling of how many deaths and hospital admissions would be prevented by various eligibility criteria for free Autumn boosters. This seems to be entirely driven by a cost – benefit analysis (kept secret) couched in purely financial terms. They are not saying it will prevent all deaths or admissions.
The JCVI work takes no account of the extra pressure on the primary healthcare system – that’s GP practices, urgent care centres and A and E departments of already seriously ill people coming forward suffering from Covid-19. Any government interested in reducing pressure on Gp’s and A and E departments is playing Russian roulette by approving these proposals.
No reason for deviation from annual flu vaccination
No rationale is given for why criteria for entitlement to a free Covid-19 jab do not mirror those in place for the annual influenza vaccine programme (those over 65 or with a chronic condition are entitled to a free flu jab).
Ignores wider range of health, social and economic benefits
The focus is on very narrow criteria of preventing hospitalisations and deaths and the proposals ignore the wider range of health, social and economic benefits (eg sickness absence, withdrawal from the labour force) of vaccinating a bigger percentage of the population. It is true that the scientific community are divided on the question of whether boosting people reduces transmission of the virus – but there is high agreement on the point that boosters reduce the chances of becoming seriously ill with Covid-19.
Inconsistencies with criteria for antivirals
The proposals are out of line with NICE guidance on who is entitled to costly (£1,000 per dose) antiviral treatments if they catch Covid-19. This recommends that people over 70 and those with chronic conditions be given antivirals.
Ignores potential to reduce incidence of Long Covid
Covid-19 vaccination has been shown to reduce the chances of developing Long Covid, yet no account is taken of the increasing evidence of the costs to the economy (many billions of pounds) of the growing incidence of Long Covid and the rate of early withdrawals from the labour market.
Ignores benefits to new borns of vaccinating pregnant women
No account is taken of the demonstrated positive impacts that vaccinating pregnant women has on the health of new mothers and new born and very young babies. Babies under 6 months are more likely to be admitted to hospital with Covid-19 than many older age groups, yet it is a travesty that the entitlement to a Covid-19 vaccine is being withheld from pregnant women – see a paper published in the Conversation and elsewhere last November. We know for example that hospital stays with new babies have a negative impact on parents – sometimes resulting in PTSD which will in turn have consequences for the economic productivity of new parents.
Ignores consideration of how Covid-19 spreads
As usual the JCVI committee deliberations assume people exist in a vacuum and their paper does not contain any analysis of how Covid-19 spreads to clinically vulnerable/clinically extremely vulnerable people and why this is significant. This is particularly pertinent to me. The proposals would mean that as a household member of someone who is at significant risk (because of underlying conditions and a failure to mount a significant response to Covid boosters) I am no longer entitled to a free Autumn booster. This is despite the fact that the person I live with will receive a free booster even though they mount little or no protective response from Covid-19 vaccines. Neither does the JCVI consider issues such as if informal carers become seriously ill with Covid-19 who is going to care for the person they look after?
Not vaccinating Healthcare workers will increase staff absence and reduce confidence in the safety of healthcare settings
The failure to vaccinate healthcare workers will further undermine confidence that healthcare is safe to access. It will also only serve to fuel sickness absence in the NHS at a time when staff are significantly stretched.
Potential to undermine messaging on the importance of vaccination
It can only serve to undermine messaging,such as it is about the importance of vaccination against serious diseases more generally.
Private Vaccines are unaffordable
Private Covid-19 vaccines are expensive – typically around £100 per dose (compared to £20 for a flu jab). The assumption is that if CV people want a boost they can pay for one yet £100 per person is beyond the means of most clinically vulnerable families.
Supplies may be deterred due to cost
The expense of Covid-19 vaccine is reducing demand which in turn is also deterring providers, particularly in remote locations, from providing the vaccine. This is leading to clinically vulnerable people having to deploy great effort and tenacity in tracking down availability and sometimes having to travel long distances to get protected. And there is no central information system on where vaccines are available except for vaccines offered by pharmadoc.
Concluding Comments
Essentially the proposals place the UK out of step with many other countries and indeed in a worse place than the USA, despite the fact that anti-vaxer Robert Kennedy is in charge of the US health department. Although the criteria may be similarly narrow in some countries, at least they tend to offer a free Covid jab on request.
There are real fears that a new Covid variant is spreading and will peak this Autumn. This could sweep through an unvaccinated population of clinically vulnerable people and others like wildfire.
The overarching problem is of course that the JCVI proposals assume that Covid-19 is a stable, predictable, seasonal virus. A large number of scientists disagree profoundly with this assumption and the authorities need to continue to be challenged on this. Moreover, the Head of the World Health Organisation recently made the point that Covid-19 is evolving and is far from over – see the following video. The problem is that no one in power is listening and the majority of the population have been lulled into a false sense of security.
If we do not continue to fight this there will without doubt be even more restrictions placed on who is entitled to free boosters next year and beyond. I have, for example, seen a previous JCVI paper which models (no details) restricting boosters to people over 80 and immunosuppressed people over 45.
In the meantime I will be forced to buy a private Covid-19 booster this Autumn because I want to protect my husband, and to be honest I have an emerging underlying condition and I don’t want to become very ill or run the risk of developing long covid. I am in the fortunate position of being able to afford a jab without too much hassle in travelling to obtain one. However, many people cannot afford £100 each and some people are not well enough to endure long journeys by road, rail and sometimes by sea to get to a location that offers private vaccines.
This is an awfull state of affairs which could, potentially, have significant economic as well as human costs.But the significant impact on people, families and households seems to have been forgotten. Clinically vulnerable Mal reminds us of this in the following video clip from the module 3 Covid Inquiry hearings last Autumn.
A government petition from the Clinically Vulnerable Families group went live on 27 August. This is an 11th hour effort. Please sign. Thank you
Gillian Smith, a version of this post was published on 19 June 2025 – updated 28 June and 14 July 2025.
Please note : I am a volunteer for the Clinically Vulnerable Families group, though please note that the information presented here and any views expressed are my own.

Leave a comment