After a relatively quiet winter season for Covid-19 infections there continue to be signs that Covid levels in the UK might be creeping up in ‘fits and starts’. And the latest information is that the wave of Covid infections currently sweeping through China, Hong Kong and other parts of the Far East has arrived in the USA and in parts of Europe. It therefore seems unlikely that the UK will be able to avoid this. However, the situation is frustratingly difficult to judge which makes it tricky to answer the question people, and particularly clinically vulnerable people and their households are asking about whether it is safe to be taking risks? This all underlines the need for better data and, after a discussion of the current situation, the second part of this blog discusses the steps that need to be taken to bring about improvements.
Current levels of Infection in the UK
Professor Christina Pagel recently provided a good overview of the situation in the UK . Earlier today Christina also published a blog reflecting evidence on the new variant that is sweeping the Far East – NB.1.8.1.
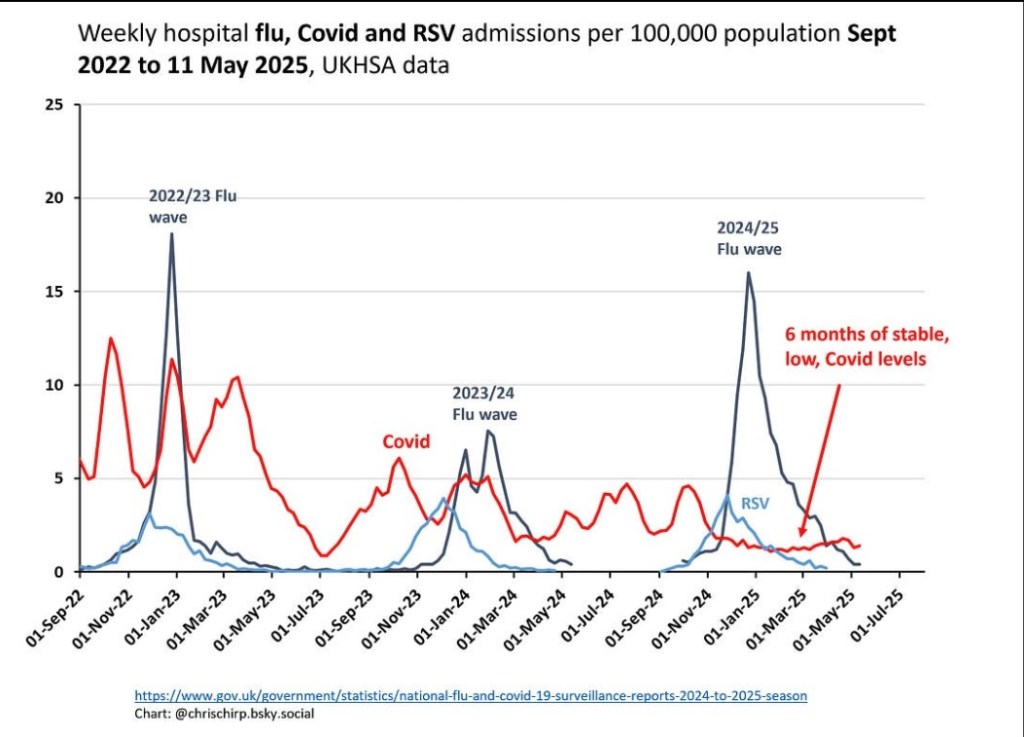
We are severely hampered in judging what is happening in the UK because the only data we have for England is the number of hospital admissions with Covid-19 and the positivity rate of patients tested for Covid-19 in hospital. There are obvious limitations to using these measures, particularly given that, as discussed below, positivity rates in hospitals do not tell us about prevalence amongst non hospitalised people, and hospital testing regimes and practices vary between areas. It is also very difficult to judge from the data whether any new variant is growing which makes it difficult to institute mitigating actions before it is too late.
Nevertheless, all the national level data we have, including wastewater data from Scotland, suggests that the prevalence of Covid-19 has been low, in relative terms, since November 2024 following what felt like a never ending series of waves seen earlier in that year.
As noted by Christina this picture is also consistent with national level waste water data from several other European countries, including Ireland, Austria, Netherlands, Finland and Belgium.
However, when we dig a little deeper into the hospital based data for England we can see that the picture is far from being the same across different parts of the country. Dan O’Hara has helpfully set out mapping data on positivity rates across different areas of England.
Of those areas reporting data we can see that there appear to be big clusters around Windsor and Maidenhead, Cumbria, Hartlepool and Sunderland.
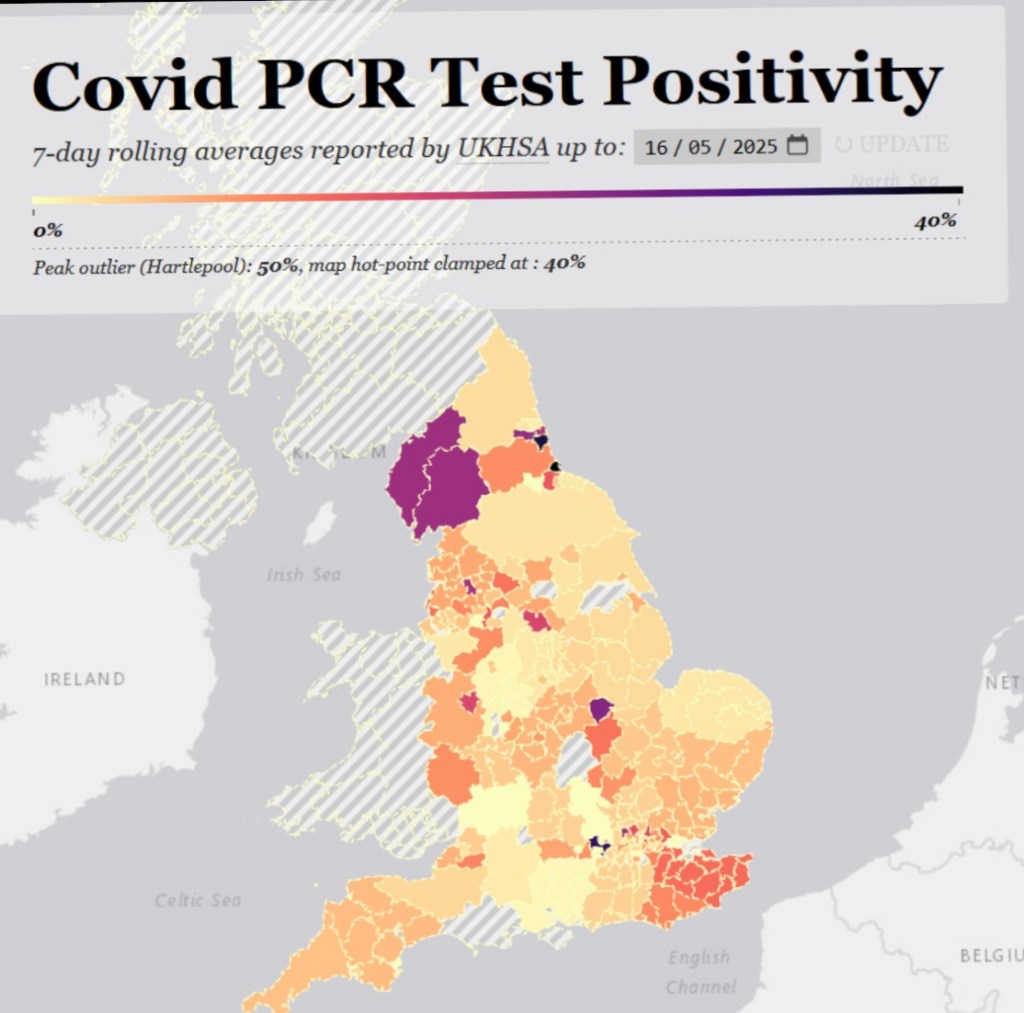
This analysis is however, partial because as noted by O’Hara, some areas have been dramatically cutting back on the reporting of data on test results.
This surely serves to reinforce the point made above, that we should not have to rely on hospital data alone as it is subject to variation in practices between different hospitals.
So is Covid-19 becoming less severe?
This is the question on everyone’s lips and the answer is it seems very unlikely. As noted by Christina Pagel above, in the absence measures to control it, the virus is still mutating. The emergence of the BA.3 variant in South Africa is an interesting case in point. We thought we had seen the back of the BA variants (BA1, 2 and 5) in 2022/23, but BA.3 now appears to have been been evolving quietly and significantly in someone with a chronic Covid infection – most likely an immunocompromised patient, and it has started spreading to other people. And now we have the reemergence of Covid-19 across several densely populated Asian countries and all the signs are that it has arrived in the USA and Europe.
The key factor influencing whether a big wave occurs is of course what happens when the virus interacts with real people. Most people will now have come into contact with various variants and or been vaccinated against them. So should we begin to hope that the much lauded ‘herd immunity’ is upon us? In other words, whilst Covid remains as a threat future waves will be far smaller. This seems unlikely given the big waves witnessed in 2024. In fact the situation may well get worse particularly if we are hit by a variant that can evade immunity. The continuing narrowing of restrictions on who is eligible for a Covid booster combined with falling take up of the offer of a vaccine may also throw cold water on the idea that Covid-19 is in decline. In a thread on X published last week, Professor Stephen Griffin, co-chair of Independent Sage took on a medic who was making the often spouted claim that : ‘COVID is a cyclical viral disease. It will keep coming back, like some other viral illnesses, But .. it is no longer a destructive force’.
Key counter points made by Stephen include:
– SARS2 waves are still driven almost entirely by virus evolution with very little influence from extraneous factors. Hence, it remains unpredictable, not cyclical;
-The dynamics between viral variation and immunity dictate the scale of epidemic waves as well as severity;
– However, as we are seeing yet again in SE Asia, when balance favours the virus, there is no doubting the additional health burden.
-I stress that this needs to come from the top down, as we are told relentlessly by @WHO, vax means many of us can, as you say, operate essentially normally in many ways. But, every infection is a roll of the dice, and #LongCovid continues to grow despite “mild” initial infection.
-But, there remain a large number of people unable to mount a vaccine response, who remain essentially stuck in 2020 as we all “get on with it”. They are marooned by the lack of societal mitigations, the politicised attitudes to masks, vax, etc, and farcical IPC ignoring aerosols’.
-Until we realise that Covid pandemics appear different to previous influenza’s, that chronic disease is under recognised and impacts many more people than Governments will accept, and that viruses are held in check by immunity rather than “becoming milder” this will continue’.
The need for better data is overwhelming
Regardless of whether Covid is increasing or decreasing the need for better data is clear. The NHS needs to plan for emerging variants and people, including clinically vulnerable people and their households/ families and friends and those at a higher risk, need to be able to judge the relative risks at any given point in time, in any given place.
The ideal would be to reintroduce a version of the original Covid-19 Infection Survey ie a random probability survey based on PCR testing with sample members offered incentives to participate. This would of course be expensive but there are a small number of possible and acceptable compromises that could be made.
However, there are question marks over whether it is sensible to attempt to cut back significantly on quality in order to save money given the experience with the winter infection survey that ran between Autumn 2023 and early spring 2024. In particular, as the survey progressed, significant doubts arose around whether it continued to be based on a truly representative sample and this was compounded by a lack of transparency over the weighting applied and the analysis undertaken by UKHSA.
The fact is that designing and executing reliable surveys requires specialist skills and appropriate resources. It is simply not true that something cheap ‘quick and dirty’ is better than nothing. It isn’t and it is usually best to do something different than a bad survey, not least because of the high risk of generating misleading results.
Overall, my judgement is that it would be a struggle in the current financial climate to argue the case for the kind of high quality survey that would be needed to measure the prevalence of Covid-19 accurately. We therefore need to be find an alternative or alternatives.
The reintroduction of wastewater analysis with timely reporting and which allowed for fine grained analysis at the local level would seem to offer greatest potential going forward.
Of course wastewater analysis is far from being the perfect solution and there are pros and cons as set out in an article from Keck and Berry 2023 and summarised in the diagram below.

Keck and Berry 2023
The key strengths are that wastewater analysis does not require expensive population survey work, and is potentially a cost effective way of gathering information on the prevalence of diseases. It also provides opportunities to cover several diseases, for example, in 2022 wastewater testing picked up a spike in polio in parts of London which led directly to a push to vaccinate all children living in London. On the other hand there are weaknesses with using wastewater analysis not least that people shed different levels of the virus – though there is thought to be clustering around the average. It also can’t identify individuals and can be impacted by transient populations.
Concluding Comments
In the face of a likely incoming wave of Covid-19 I strongly recommend that wastewater analysis be reinstated across the UK, with regular, up to date publication of findings broken down by local area as far as possible. This would enable clinically vulnerable people and their households and others to gauge respective risks at different points in time.
In terms of what the existing data trends mean for how we behave right now – I would urge some degree of caution. This is because it is too early to judge what is happening, Covid-19 has not gone away and those who are clinically vulnerable often have weakened immune systems and lack of a full response to vaccination which make them more susceptible.
However, my personal view (please not this is not my area of expertise) is that if you have not already done so, get those appointments eg opticians, dentists, that need to happen out of the way soon and to take some measured risks with appropriate mitigations bearing in mind the Swiss cheese model discussed in my blog on how to avoid catching Covid. What taking measured risks means in practice will vary between individuals and households, but until we adopt the kind of measures seen across Japan – including information on CO2 levels (see photo below of an indoor cinema complex – just image how much freedom we would have with this kind of information system) – the risks will sadly remain high.

We also need to work to counter the kind of anti vaccination messaging currently taking place in the USA gaining ever more traction in the UK. A good summary of what the anti vax movement are claiming and the counter to this appeared on Channel 4 recently and I will be returning to this in a subsequent blog post.
Gillian Smith
25 May 2025

Leave a comment