
Covid Inquiry
The last three weeks have been very busy at the inquiry with 48 witnesses plus opening and closing statements from core participants crammed into twelve and half days of hearings. Issues covered included:
- How vaccines and treatments were developed and the enablers and barriers to this, including speed and safety issues;
- issues with the roll out including logistical issues and prioritisation;
- evidence on the life saving impacts of Covid-19 vaccines (overall it is estimated that 123,000 lives were saved during the time period covered by the inquiry – up to mid 2022) ;
- The relatively small number of people damaged by vaccines, including the AstraZeneca vaccine and issues around the stigma these people face and inadequacy of the compensation scheme for these families;
- Issues around vaccine hesitancy and misinformation and ways of countering this;
- the successes and failures of reaching certain Black and Minority ethnic groups, Migrants and Gypsy, Roma and Travellers communities to name a few;
- the developments of treatments for people with Covid-19;
- the fraught issue of the failure to provide prophylactic treatments for immunosuppressed and other people who could not take or mount a response to the vaccines (discussed in the next section);
- assessments of the UK’s readiness for the next pandemic, including in terms of ability to develop and manufacture vaccines and therapeutics.
As usual Jim Reed has done a good job in producing weekly podcasts overviewing the proceedings – listen to podcasts published on 18 January (including the appearance of Lara Wong, Head of CVF); 25 January (including the appearance of Dame Kate Bingham); and 1 February.
Clinically Vulnerable Families
The appearance of Dame Kate Bingham, former head of the Vaccine Task Force was one of the key highlights for the CVF group and is captured in a thread of short clips here.
Dame Kate exposed what many clinically vulnerable people have been saying for years – namely that the UK government failure to provide clinically extremely vulnerable people with protection against Covid-19 through prophylaxis drugs such as evusheld was because that there was a two tier system operating within Whitehall which essentially ignored the needs of clinically vulnerable people to live their lives. Put starkly, the government were unwilling, on cost grounds, to buy treatments for the CEV in complete contrast to the, at times risky, efforts to develop and procure vaccines – see the following video clip which captures one of the key points made by Dame Kate.
Yes, it is true that the issues are more complex than for vaccines, and the cost per dose higher – £100’s rather than £10’s, but many other developed countries bought the drug for immunosuppressed people who were then able to enjoy the same freedoms as vaccinated people at least until evusheld became less effective with the arrival of the omicron variants.
The depth of bitterness felt about this issue cannot be underestimated, not least because of the subsequent messaging around ‘freedom day’ following the opening up of society post vaccination and the abuse and ridicule suffered by clinically vulnerable people, who were left at significant risk, that ensued.
The other key highlight was, of course, the appearance of our very own Lara Wong whose evidence is captured in this thread. Lara highlighted how some clinically vulnerable people fell through the cracks due to limitations in health data and had to fight their own corner in gaining access to vaccines and treatments. Lara also highlighted issues around the safety of some vaccination centres, and also called for a range of anti viral treatments to be available as some existing treatments are not suitable for people with certain conditions. She also majored on some of the key issues around evusheld referred to by Dame Kate Bingham and outlined some of the consequences for clinically vulnerable families – see the video clip below.
Lara also discussed the often forgotten issue of clinically vulnerable children, who often had to wait for extended periods of time to receive any protective vaccines or treatments – see the video clip below.
And finally, a nice comment from Baroness Hallett about the role of CVF in lobbying on the need to keep the hearing centre safe to attend eg through ventilation and air filtration.
In the CVF closing oral statement on 31 January, senior barrister Adam Wagner gave an overview of the issues highlighted by CVF across the module both in statements and questions – please find the video clips covering the entire statement here. See in particular the first video clip from Adam reproduced below.
The UK Government Machine – delivery and innovation
The Covid Inquiry has witnessed some outstanding examples of government officials and Ministers who played a pivotal role during the period covered by the inquiry, but also many examples of apparent low expertise, bureaucracy, and lack of pace resulting in poor advice to decision makers, wrong decisions, and delays.
This was one of the issues covered in the evidence given by Dame Kate Bingham and others. To counter the lack of expertise needed to deliver on the vaccine programme was a key reason for the independence, freedom to bring in expertise, budget and a direct reporting line to the PM afforded to Dame Kate. Indeed, these were conditions she insisted upon before taking up what she knew would be a challenging role as head of the Vaccines Task Force. The story is well documented in Dame Kate’s book The Long Shot.
I recognise many of the things Dame Kate says from my own time working in central government departments in Whitehall. In particular, the lack of emphasis on scientific expertise, including social science skills, stands out. In fact I would say, with a few notable exceptions, there was and still is a lack of emphasis on expertise at all, except of course a certain brand of economics and certain areas of policy requiring engineering skills.
The lack of real world experience, including in business skills is also clearly in evidence and is a particular bug bear of Dame Kate. Indeed, to get on in the civil service one needs to move around posts and departments sometimes with ridiculous frequency, the overall goal being to create the good ‘all rounder’.
This in turn leads to systems for advancement that place emphasis on the range of experience that candidates have, which is often seen as more important than expertise to do the advertised job. And again this can lead to external recruitment decisions in which officials select people ‘like me’ who can be ‘trained up to be like me’. This is no doubt a gross oversimplification but I could go on at length!
Poor decision making in government is of course often the fault of politicians who sometimes insist on policies that it is clear won’t work, unrealistic timetables, coupled with an un- willingness to take account of evidence and arguments even when they are given good quality briefings from officials .
However, it is often also the fault of officials working in central government who lack a historical memory about previous policy attempts to address issues, and who may be too focused on reaching what may be seen as a logical way forward (the kind of conclusion one might reach in an Oxbridge debating society perhaps). Alternatively they might be looking for something they regard as easy to deliver or perhaps something politicians want to hear. Or they might not have much idea of how what they are recommending will be delivered in practice, but it sounds good and might generate a lot of outputs. What was evident from my time in Whitehall was a general unwillingness by policy officials to tell Ministers that their timetables were too short, and funding streams insufficient given the ambitions, but of course to do this one would need the expertise to actually know this and to convince Ministers of it.
If this is indeed what is happening it comes at the expense of completely honest briefings underpinned by the right arguments, evidence, evaluation evidence (except a very narrowly focused kind of economic evidence), and delivery considerations all geared to achieving real workable outcomes – not simply outputs which make it look like something useful is happening.
I for one would have loved to have been a fly on the wall at the decision making processes leading up to the announcement not to go ahead with a £450 million investment in the AstraZeneca Vaccine Plant on Merseyside which comes against a backdrop of other closures and cutbacks.
In particular I would love to know if the Minister taking the decision was made aware of what several witnesses told the recent Covid Inquiry module 4 hearings, namely that the UK is possibly in a worse position now than at the start of the 2020 pandemic. This included Dr Clive Dix, former Deputy chair of the Vaccine Task Force, who stressed that it was essential to have the expertise and manufacturing capacity within the UK.
This also chimes with the key messages in a recent House of Lords Science and Technology committee report in which concerns are raised about the UK’s ability to develop and manufacture vaccines in a future pandemic. Remember, we do not know what the next pandemic will look like nor what type of vaccine will be needed, yet the government seems to be putting all its eggs in one basket by negotiating a 10 year contract with Moderna. In a letter to the Chancellor of the Duchy of Lancaster the chair of the committee said:
The Committee’s headline message is that the UK must have a resilient, diversified domestic vaccine manufacturing sector, from research through to clinical trials and large-scale manufacturing. This is a critically important sovereign capability for security against the next pandemic. Recent developments raise concerns, and the sector needs renewed focus and government support to ensure that lessons are learned from the COVID-19 pandemic and capacity retained.
The Department for Health and Social Care (DHCS)
The key department which Clinically Vulnerable People rely on is DHSC and its agencies. It is therefore concerning that there has been so much criticism from two House of Commons Select Committee chairs about a recent report and subsequent hearing
Early last week a report from the highly influential Public Accounts Committee reported significant concerns about the lack of ambition and clear ideas from officials. In particular:
‘Government’s NHS ambitions run counter to officials’ lack of ideas or drive to change. In a report published today, and in the context of a worsening financial position for the NHS, the Public Accounts Committee warns that, while Government’s forthcoming 10-year plan will be essential to the health service’s recovery, senior health officials seem to be unambitious when it comes to taking the radical steps to begin to implement it.’
In commenting the chair of the PAC goes on:
‘We were aghast, then, to find amongst senior officials in charge of delivering these ambitions some of the worst complacency displayed to the PAC in my time serving on it. ‘
“The evidence given to our inquiry exposes the perennial weaknesses with which those scrutinising this country’s health systems are now very familiar. We therefore have a simple message for those senior officials responsible for delivery. Truly fresh ideas and radical energy must be generated to meet the scale of what is required – on community healthcare, on prevention, on digital transformation. Given the position of the NHS, forcing this Committee to wade through treacle by mouthing the same stale platitudes of incremental change is simply not going to cut it.”
Drawing on the findings and a subsequent hearing the chair of the Health and Social Care select committee Layla Moran commented along broadly similar lines following a session with NHS leaders:
“Following today’s report by the Public Accounts Committee, this morning’s evidence session was an opportunity for NHS leadership to prove their drive and dynamism.
“Regrettably, we were left disappointed and frustrated.‘
“We had hoped for a sharpness in witnesses’ responses but were exasperated by the lengthy and diffuse answers that were given to us and will be writing to them to seek the clarity that we expected to hear in the evidence session.”
It is not all bad news though! On a brighter note and in other news over the last two weeks or so it was announced that Dame Jenny Harries will be stepping down as Chief Executive of the UK Health and Security Agency (UKHSA) in the early summer. Dame Jenny’s expressed views include that the UK should be more like Sweden in a future pandemic, and her statements on the lack of evidence on the superior protections offered by FFP2 and FFP3 masks compared with paper masks etc lack substance. We hold our breath regarding who is appointed to replace her as this will give a clear indication of whether the government is serious about delivery and has plans any change in priorities and messaging at the UKHSA.
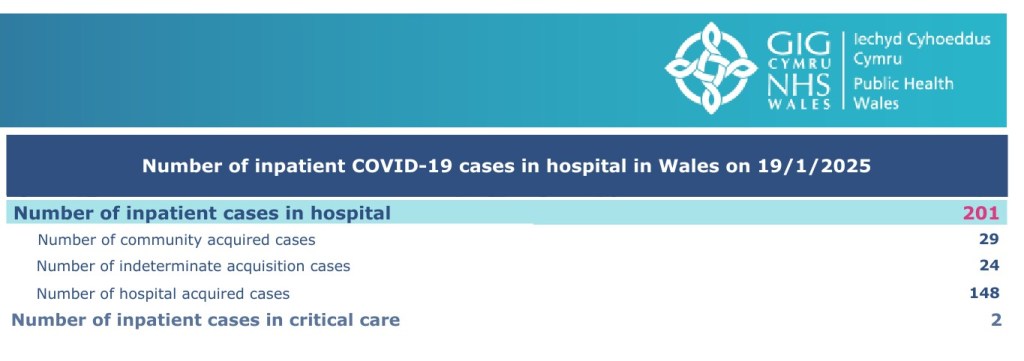
The continued urgency of the need to improve Infection Prevention and Control measures in medical settings was also laid bare recently when data was released (see below) showing that no fewer than 73% of people in hospital in Wales with Covid acquired Covid-19 in hospital whilst being treated for something else. Indeed, this is exactly what happened to someone I knew 18 months ago. He caught Covid after being admitted to hospital and went on to die of Covid. It is surely only a matter of time before UK governments grasp the issue and make strong efforts to improve infection prevention and control measures – or maybe I am being optimistic at the moment?
The USA
The actions of President Trump to date are deeply worrying. In particular, the day one order to pull the USA out of the World Health Organisation. This action has attracted numerous adverse commentary including from former Foreign Secretary, David Miliband and former Prime Minister Gordon Brown who outlines the wrongheadedness of the decision in a world where global co-operation needs to increase. Specifically on Covid, he comments:
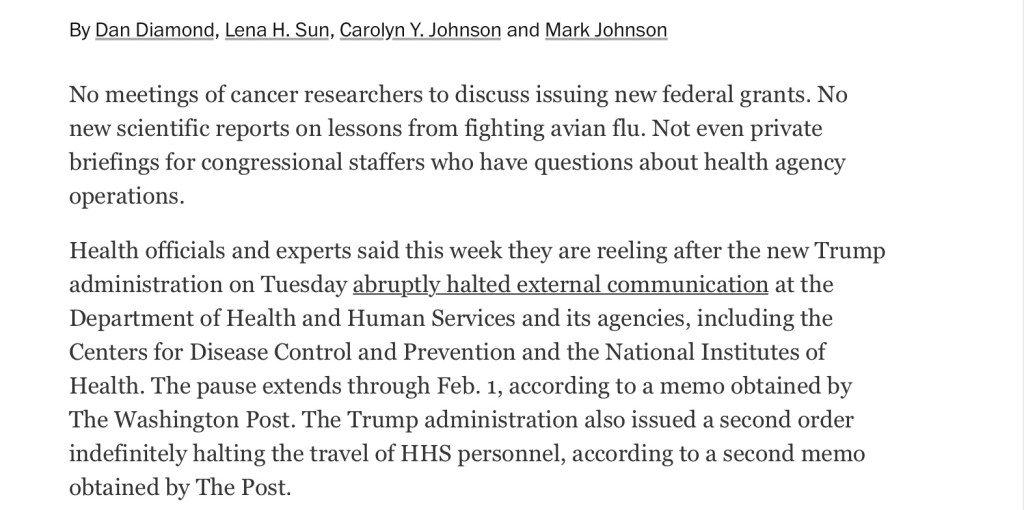
It has also emerged that President Trump has ordered a temporary ban on communications, including meetings between cancer researchers, new scientific reports on lessons for fighting avian flu and more. According to the Washington Post (see screenshot below) this is to allow the new team to set up processes for review and prioritisation.
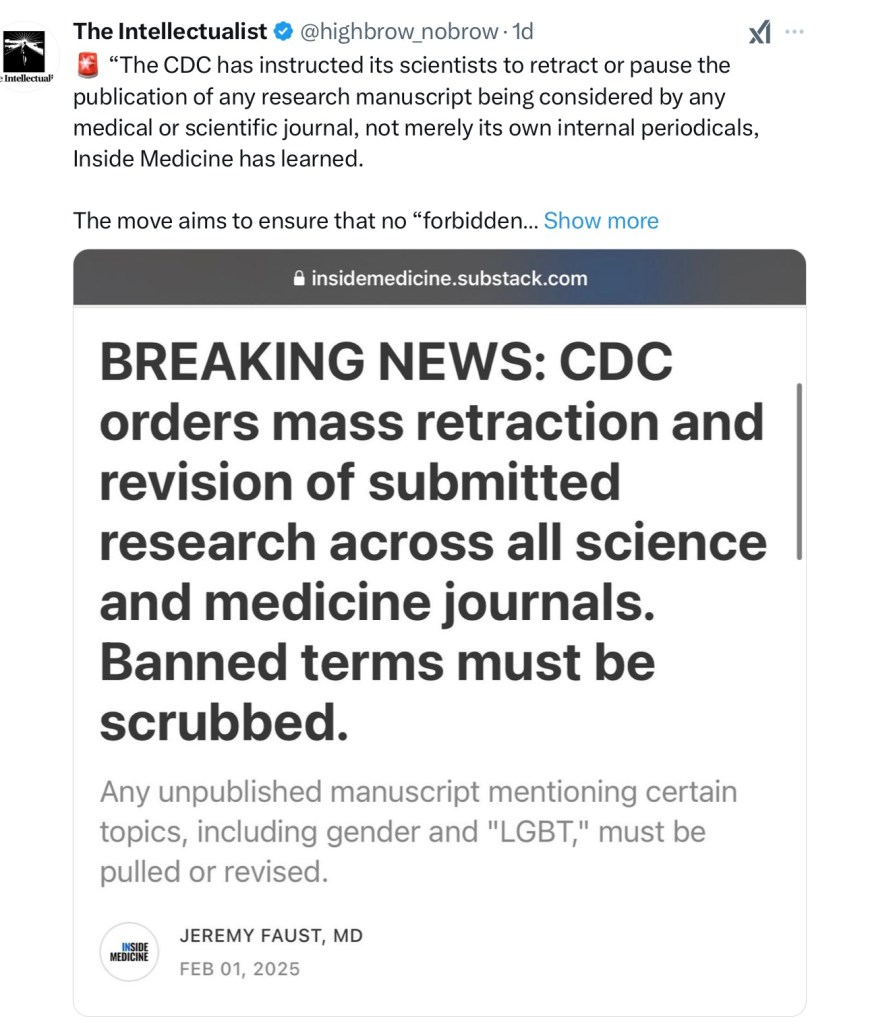
And it is clear that the new President has ordered significant deletions from and tampering with the world respected Centre for Disease Control website. This level of doctoring of the evidence that is available to the public will no doubt gain pace in the coming weeks and months. If you have not done so already you are advised to download and save anything you wish to save for future reference.
Concluding Comments
Clearly a great deal has happened since the turn of the year and this blog is an attempt to provide an admittedly partial overview of events from the Covid Inquiry and elsewhere, written with a particular interest in the position of Clinically Vulnerable Families.
Gillian Smith
3 February 2025
NB I am an active member of the Clinically Vulnerable Families CVF group and am closely involved in supporting our role on the inquiry. However, as is pertinent to all blogs on this website, and as highlighted on the homepage, what I write here is not an ‘official’ view and does not necessarily reflect our policy on all matters.

Leave a comment