Summary
Back in 2020 and 2021 it was normal for people in the UK to wear masks, and it was sometimes mandatory in healthcare, supermarkets and other public buildings, for example. However, after the so called freedom day in July 2021 fewer and fewer people wear masks, even in very high risk settings which has proved to be problematic for many people, including the clinically vulnerable and their families.
From late 2021 onwards instances of mask abuse and mask discrimination have without doubt grown. This is a big problem, particularly for people who have not responded to the vaccines and for whom masks are a vital layer of protection against a virus that can kill or cause serious illness.
Who would have thought that wearing a piece of paper or fabric on your face would cause so much angst? But it has and is perhaps a wider indication of government communication and policy failures throughout the pandemic.
This blog discusses the different kinds of mask abuse and mask discrimination occurring in the UK at present and draws out some points for future action.
Reminder of why masking is important
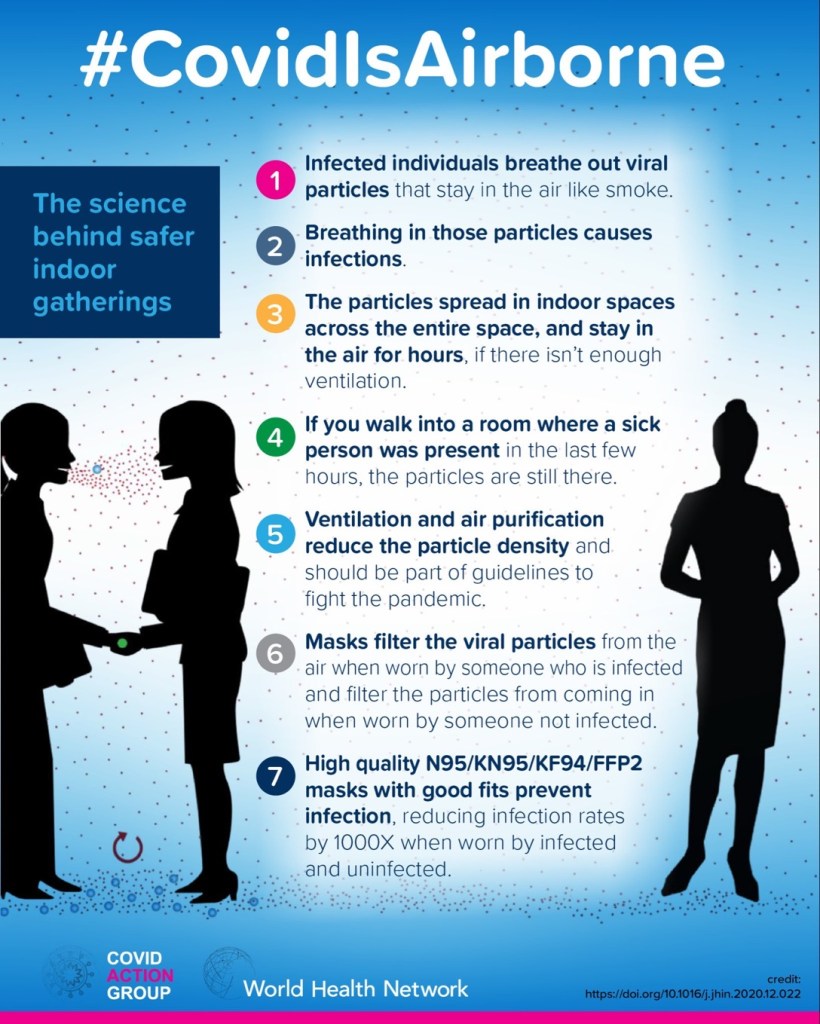
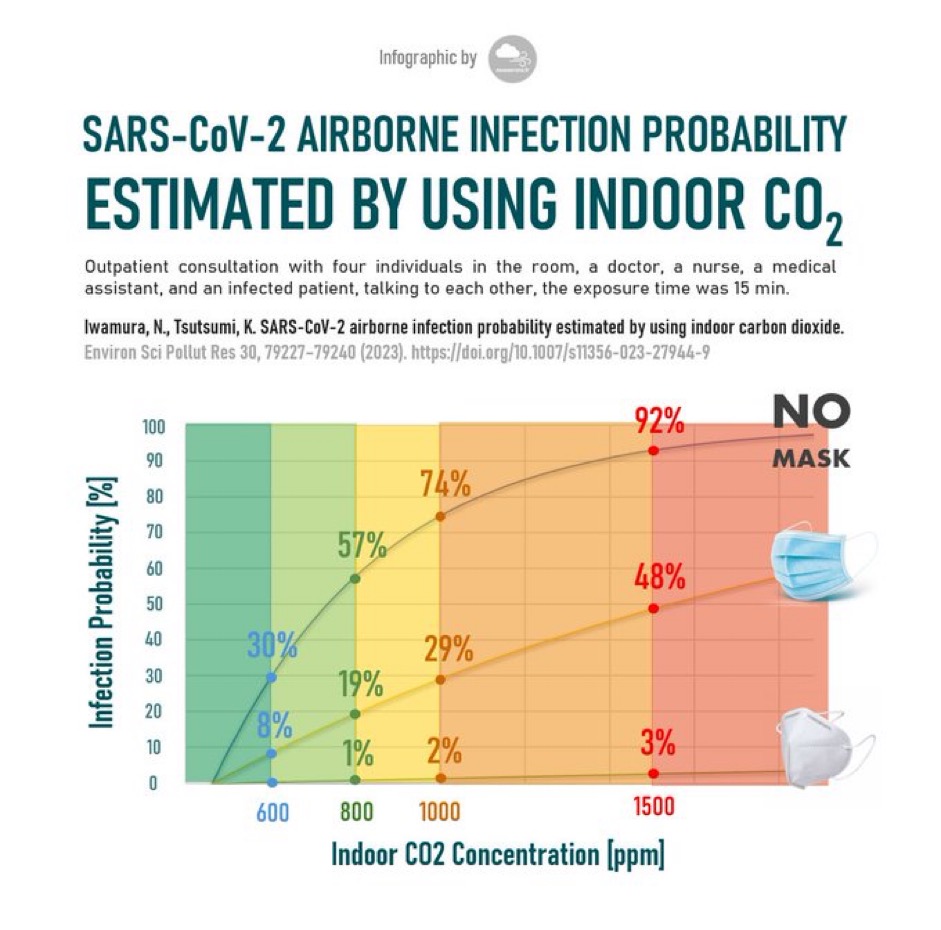
My blog on Avoiding Covid section 3 i. explains why it is important to wear a mask, particularly in unventilated indoor settings where the CO2 concentration is likely to be high. Covid-19 is an airborne disease. Unlike illnesses transmitted via droplets, it can hang about in the air for hours, remain infectious and infect people.
Due to its aerosol like mode of transmission the type of mask you wear is very important. As illustrated in the diagram below an FFP2 or FFP3 ear loop mask is far more effective than a paper surgical mask and an FFP3 that goes all the way round the head such as a 3 M aura mask is even more effective. Again this is discussed in greater detail in my blog on How to Avoid Catching Covid.
There is a great deal of misunderstanding around the importance of wearing a well fitted, preferably un-valved mask/ respirator. There are a large number of people, including some scientists, who want to discredit the effectiveness of mask wearing for political reasons, and indeed, highly misleading evaluations have on occasion be published which were subsequently found to be biased. Again this, including the Cochrane saga, is discussed in my previous blog on Avoiding Covid.
Another common misunderstanding is that wearing a mask only protects other people – not the person wearing a mask. This is untrue. If you wear a mask, particularly an un-valved good quality mask (FFP2 or FFP3) you will be providing yourself with a great deal of protection as illustrated in the diagram below.
How extensive is the problem of mask abuse?
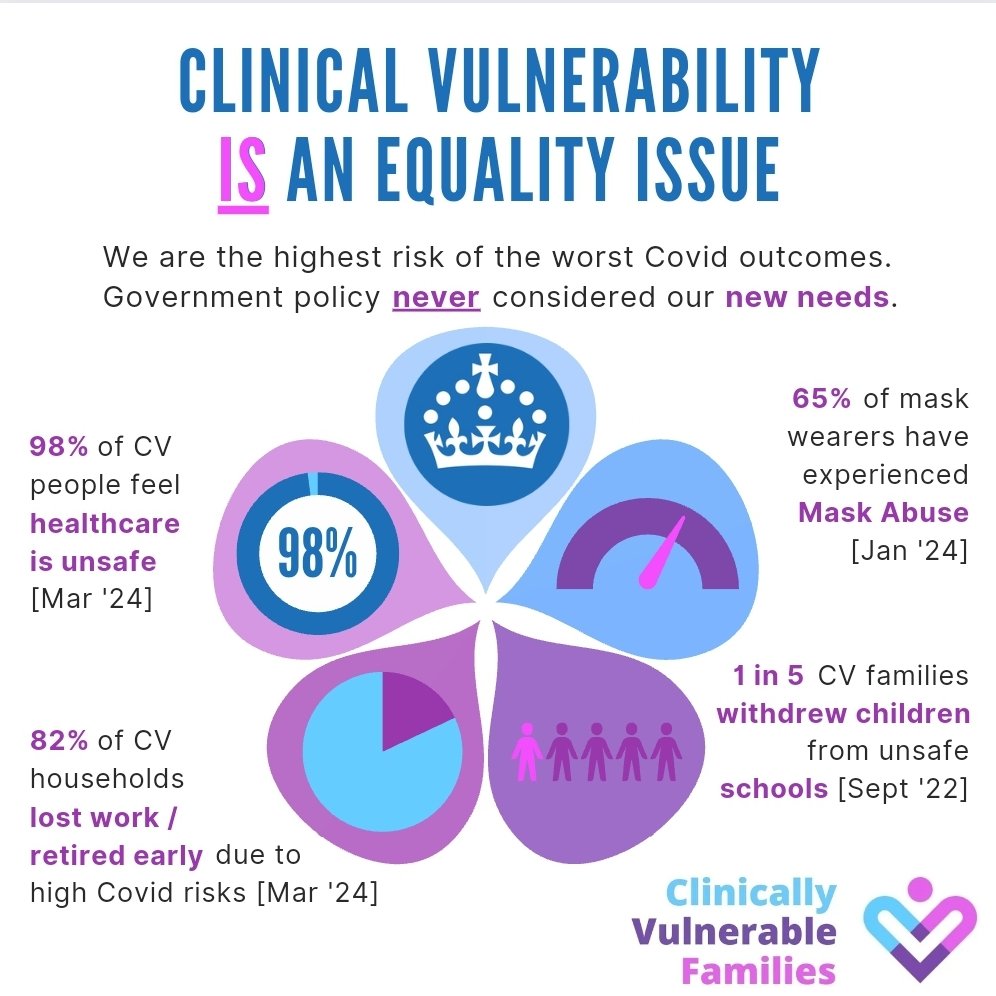
A recent survey of clinically vulnerable families found that as many as 65% of people surveyed had suffered some form of mask abuse. This is in sharp contrast to the situation in many other countries – particularly in the Far East where mask wearing outdoors and indoors is considered normal behaviour. Indeed, one can observe this in central London everyday as the tourists from these countries routinely walk around masked.
Types of Abuse
Everyday occurrences in shops/services, on public transport, in the street
Mask abuse ranges from everyday behaviours like starring, verbal and non verbal jibes such as shouting, shaking heads, pretending that the masked person is not audible as well as deliberately coughing over them. This can be very upsetting to the person on the receiving end, many of whom are ill or vulnerable and, on occasions, drives them back into their homes. This is discussed further in my blog on Avoiding Covid. It is particularly distressing that some children and young people are regularly subjected to mask abuse, including the case of a young journalist from Northern Ireland who wears a mask in order to protect others in her household.
Medical Settings
Other more specific examples of abuse include medical staff making the masked person feel uncomfortable, interrogating them about why they wear a mask, and providing false information in order to attempt to provide reassurance as in the recent BBC Casualty episode which many of us have complained about.
It is also apparent from a recent example that mask discrimination is present in some medical schools. In this example a CVF member who is a clinically vulnerable medical student lost marks because she wore a mask during an exam.

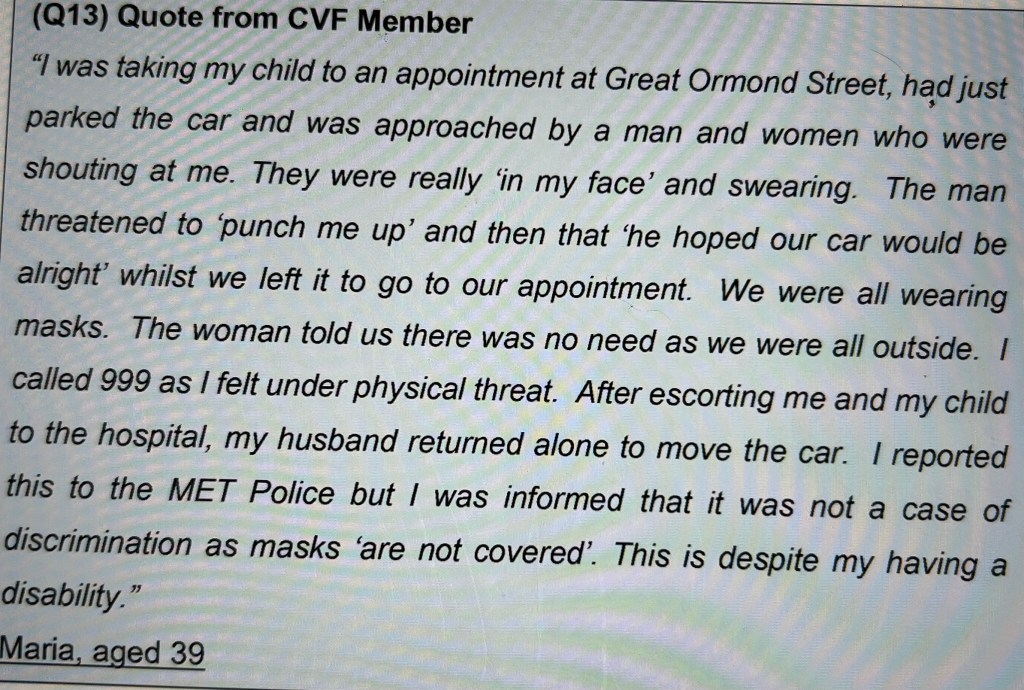
Incidents sometimes also occur outside medical settings when people are masked up ready to enter hospitals. In the example below CVF member Maria who is disabled had to call 999 because of an incident outside Great Ormond Street hospital in London that occurred when taking a sick child to hospital.
Schools and Colleges
There are also many examples of particular school teachers mocking masked children during lessons and pretending they cannot hear them, even though they are perfectly audible. This can also lead to bullying by other children.
Although there are some examples of schools that handle this issue well, antagonism to mask wearing is thought to be a key reason why as many as 1 in 5 clinically vulnerable people surveyed had withdrawn a child from school.
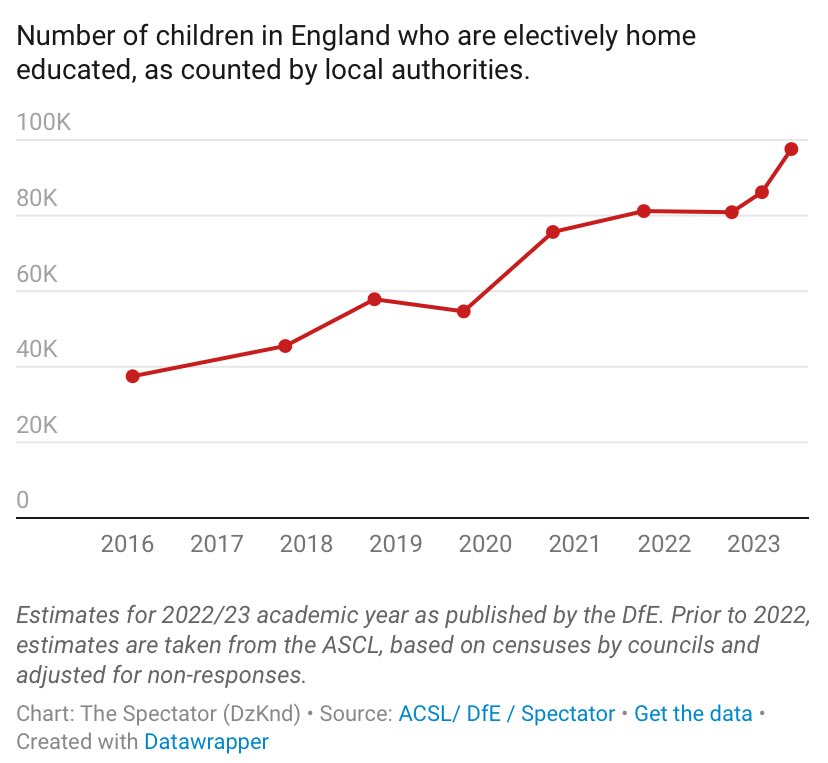
Home education and on-line services to support this have ballooned in recent years and a key driver of this is that parents consider, usually correctly in my assessment, that schools without proper ventilation and air filtration are unsafe.
Employment Discrimination
We also know that employment discrimination based solely on whether someone wears a mask is a growing problem. This is a key reason why the clinically vulnerable and their families search out home based roles even where it involves a cut in salary. Examples of employer behaviour include objecting to those in public facing roles wearing a mask because it ‘would make customers feel uncomfortable’. There are also examples of this argument being used in back office roles along the lines of ‘it would make your colleagues feel uncomfortable’ or ‘no one would be able to hear you’.
There are also particular issues in education and it is thought that many high quality teachers have left the profession because schools are unsafe and people object to them wearing a mask to protect themselves and their families.
A stark example of these issues is described by a member of the CVF families group in a recent blog. This very sad and enraging story which recounts what happened at four job interviews. It demonstrates just how far some employers will go to avoid employing someone simply because they wear a mask. Indeed, from reading this one would never guess there is a shortage of teachers, and a high sickness absence rate in this country. Indeed, a recent report of the Winter Covid-19 Infection Survey concluded that those working in education were particularly at risk of testing positive for Covid-19.
Democracy

There are also particular problems around voting in elections which pose a direct threat to the ability of clinically vulnerable families to participate in democracy. CVF member Andrea Barrett who had a heart transplant when she was a young child launched a crowdfund in order to cover the legal fees involved in bringing a legal case challenging the Voter ID law under the Equality Act 2010 and the Human Rights Act 1998, arguing for our rights to participate in democracy fully and safely (this has subsequently been dropped and Andrea has used the funds raised to buy HEPA filters to donate to schools).
The background is that new photo ID rules brought in just before the May 2023 elections require that voters must show photo ID and the Electoral Commission states that when voting in person, staff members will request to see the ID and check that it looks like the person presenting it.
In 2023 Andrea says she took along her passport, along with a video of herself putting on her mask, to the polling station but was met with general hostility and told she could not vote unless she removed her mask so they could see her face.
In response to this case the All Party Parliamentary Group (APPG) for Democracy and the Constitution has said:
“Given that the passport was genuine and valid and that the photograph did not give rise to reasonable doubt that it was consistent with what could be seen as Andrea Barrett’s face, there is a question as to whether the refusal to allow her to vote was lawful under the 2022 Act (and, indeed, various provisions of the Equality Act 2010).”
And speaking to the i. newspaper, Lara Wong, founder of Clinically Vulnerable Families added:
Lara Wong
“Andrea’s case highlights the Government’s neglect in recognising new equality issues and accessibility needs faced by clinically vulnerable people, which were evident since Covid’s emergence over four years ago.
I understand that this has all led to Eastleigh Council apologising to Andrea about her treatment. Moreover, because of pressure applied by Andrea, Hampshire introduced a county wide policy for GE 2024 whereby returning officers were instructed to do any checking requiring de-masking outside.
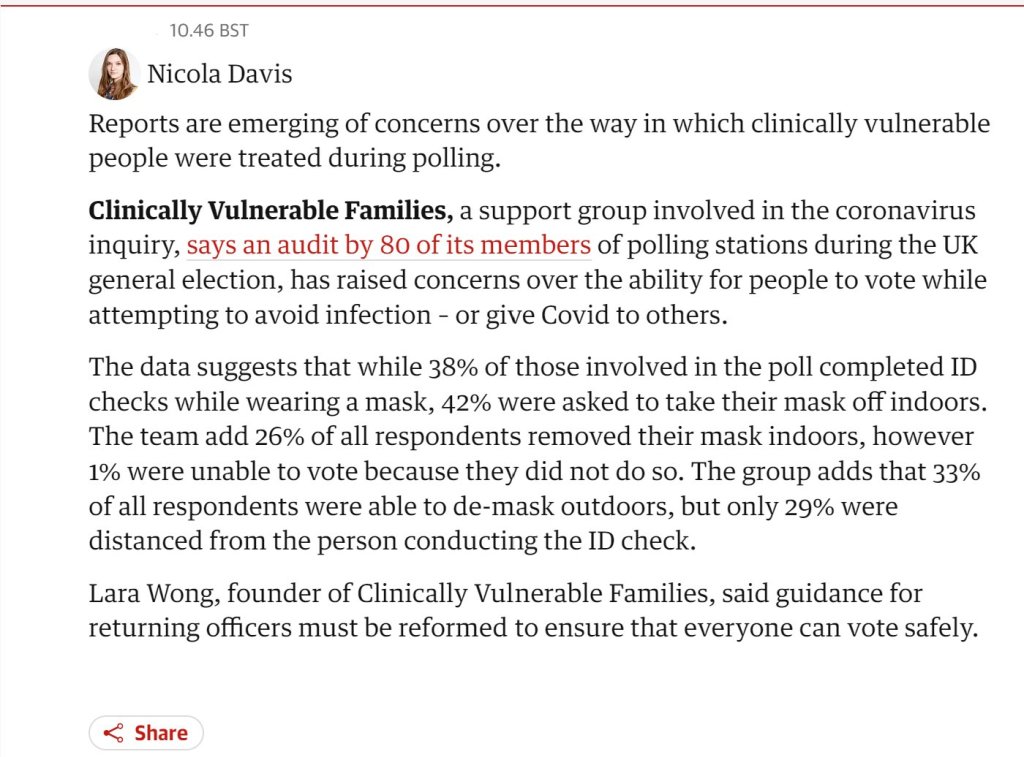
However, more generally and despite early optimism that arrangements for the General Election would be appropriate, a number of continuing problems were evident, in practice. The enclosed clip from the Guardian 9 July sums up the situation. The issue has also been reported in the i. newspaper. Clearly a lot more work is going to be necessary:
Another aspect of democracy is the right to demonstrate. Clinically vulnerable people and their families certainly have plenty to demonstrate about, but new laws introduced following warnings from police chiefs that some protesters are using face coverings to conceal their identities, mean we could be arrested and face a prison sentence just for wearing a mask on a demonstration.

What are the underlying causes of mask abuse?
My blog on ‘What is Wrong with People‘ provides some clues about why people behave as they do.
Clearly there are a number of potential drivers, but explanations around psychology, combined with a general desire to forget the traumas of the pandemic, are probably key.
None of this excuses poor behaviour towards clinically vulnerable people and others who mask. People who exhibit these kind of aggressive behaviours are without doubt suffering from some serious anxiety and wider mental issues that need to be addressed.
Concluding Comments
Mask abuse tends to make people who mask feel uncomfortable and discourages them from attending events and participating in necessary appointments and social activities in general. This is bad for society and it is bad for the economy.
Of course, many of the problems we face can be attributed to poor government communications. The communications around ‘freedom day’ were particularly problematic and failed to convey the message that the pandemic is an ongoing challenge, and that some groups have particular needs and challenges. There is no doubt that this simplistic messaging is behind some of the antagonism we are seeing towards people who mask. We are a reminder that the pandemic is far from over and Covid-19 continues to pose many dangers. Some of the abusers will know this, but because they are anxious they can’t admit it and turn on mask wearers instead. This does not excuse these behaviours.
Of course, it would be less necessary to wear a mask if we had clean air in public and private buildings and the public were better educated about how to mitigate the risks from Covid-19. Again, many countries including in parts of mainland Europe and the US are surging ahead of the UK in making progress on this front, but UK policy in response to this is virtually non existent.
We can only hope for fresh thinking in UK government circles following the recent general election.
Some trades unions and professional bodies are already on board in supporting individuals who wish to pursue cases against employers about disadvantage experienced as a result of requesting reasonable adjustments and objections to mask wearing. There have been a few notable recent victories achieved by CVF members, but we need to make progress here.
We clearly need to have legal status as a particular equalities group which is embodied in equalities legislation much like disabled people. Although clinically vulnerable people have always faced barriers, covid-19 has intensified this and increased the dangers. If we had legal status we would be able to bring legal actions and pressurise the government and others into adopting a more inclusive approach based on the specific inequalities we suffer.
Specifically on masks, we believe the right to wear a mask must become a ‘protected characteristic’ under UK equality law, similar to the protection given to people wearing a Kippah, Turban, cross, Kara, or Hijab.
We are working on achieving legal status and particularly Lara Wong from CVF group who has had a recent success in getting the UK Covid Inquiry to recognise clinical vulnerability as an equality issue and allowing CVF to participate in their ‘Equalities Forum’. Overall, however, gaining full status in the 2010 equalities act is more of a long term ambition than anything that is going to change in the near future.
As set out in the concluding section of my blog on how to avoid catching Covid it is important to build our resilience and assertiveness given the challenges we face. Every situation will be different and assertiveness does not come easily to many people for understandable reasons, but there are on-line and written materials on how to work at this.
Finally, it is very important to seek support if you are struggling due to mask abuse or for other reasons relating to your clinical vulnerabilities. You might seek this from a sympathetic friend or family member or from our friendly CVF Facebook group (if you or a household member meet the criteria) and other on-line forums that have people that understand and are willing to help.

Leave a comment