
Please note this blog was updated and a revised in August 2024
The vast majority of the population of the UK have had at least one confirmed or suspected infection. But some people have never had Covid (including myself and my husband) and many have only had it once. In some cases never having Covid or one dose will be down to luck, or to some little understood aspect of the underlying immune system. However, in most cases it is explained by the mitigation measures which my household practices. This blog discusses these measures and how effective are they?
Background
Many people, including myself, argue that mitigation should be a matter for national governments and institutions and that measures should include better sick pay so that the sick can stay away from work, hence reducing the circulation of infection, and legislation and funding to support the provision of clean ventilated air in public buildings and private establishments, not least schools and hospitals.
However, despite the huge potential benefits, the fact is that the UK government, and many other governments around the world, have abandoned any national level mitigations, except for limited access to vaccinations, on the spurious grounds of ‘living with the virus’, and making individuals take responsibility for their own safety.
This is despite the fact that Covid continues to put the hard pressed NHS under pressure all year round since unlike flu it is not seasonal, waves can occur at any point in the year driven by new, ever more immune evasive variants.
It is increasingly evident that Covid infections cause a multitude of other serious conditions that are placing the NHS under pressure eg heart attacks and brain issues. See, for example the discussion and evidence presented in my post on the Tragedy of Long Covid. Over 2 million people and children in the UK are suffering from ‘long Covid’ with knock on impacts on labour shortages, the economy, lost learning and mental health.
One of the most important things that most people can do to avoid infection or to avoid becoming seriously ill with the initial infection is to get vaccinated and boosted wherever you are entitled to a free vaccine. Pfizer and Novavax vaccines are also available to buy privately via pharmadoc and Boots (Pfizer only).
We know that the vaccines don’t stop the latest variants from infecting you, though there may be some protection (estimates differ). However, for the vast majority vaccines will stop you dying from the initial infection. There may also be some protection against long Covid though we don’t know to what degree – evidence based estimates vary from as little as 15% up to well over 50% reduction in long Covid.
This paper briefly discusses vaccination before moving on to discuss mitigations people themselves can take.
1. Vaccination
There are restrictions on who has access to vaccines. In the UK the under 50’s who are not clinically vulnerable have not had access to any kind of vaccine since Autumn 2021 and the under 65’s have not had a boost since Autumn 2022. There is much debate about this but it is beyond the scope of this paper, but is discussed in other posts on this website including the Saga of vaccinations against Covid continues.
There are also problems experienced by many clinically vulnerable families, including for a member of my family, in that an estimated 2% of people don’t produce antibodies in response to the vaccine. It is very unclear what this means. Most practitioners take the view that this group are significantly more at risk from serious complications but we do not know how far t cells or other factors kick in to provide some protection. But this does not mean clinically vulnerable people should not get vaccinated. The vaccines may be offering some protection in ways that are not fully understood. It is also estimated that for clinically vulnerable people the risk of developing long Covid are many times greater than for fit and healthy people so anything that might protect protection is worth having.
It is clear therefore that vaccination on its own is not enough. This is particularly true of vulnerable people who do not respond to vaccines, but it is also relevant across the entire population because if you catch Covid you may pass it onto someone who is vulnerable and kill them. There is also an estimated 1 in 10 chance that you will get long Covid as well as a heightened risk of developing a range of other serious illnesses including brain disorders. The fact is that the UK government and its agencies is almost completely silent on these points, and does not provide any information to inform our risk assessments and mitigation measures.

The consequence is that many people and organisations, including parts of the NHS, seem to be operating with a misinformed understanding of the nature of Covid and how it spreads with significant consequences for what steps we should be taking to control Covid-19. In particular there seems to be very little awareness that Covid-19 is primarily an airborne disease, despite international scientific consensus on this being very clear. Covid can be spread by droplets but is mainly spread by inhaling virus- containing aerosols in indoor air. Therefore endless washing of hands will do very little to contain the spread of Covid (but is useful for other reasons).
Moreover, some people, even some medics, seem to be operating on the false idea that the liberal spreading of Covid infections can create a kind of ‘herd immunity’. This theory was commonly talked about early in 2020 but has since been largely discredited. Indeed, there is some evidence to suggest that rather than strengthening resistance to Covid, catching the virus may weaken your immune system but this is a complex issue. There is certainly plenty of evidence of people having Covid on numerous occasions. Yet one of the most damaging things about this is that evidence suggests you are more likely to develop long Covid the more episodes of Covid you have had.
Despite the regular moaning on twitter by people living in countries such as the US, Canada and Australia, my assessment is that the UK is one of the worst, if not the worst. Even in the US which is seen as a country which promotes individual responsibility over state action, the Centre for Disease Control and Infection has recently published clear guidance on the need for improved ventilation in buildings, whereas in Belgium all hospitality establishments are required to display the quality of the indoor air.
Individual level Mitigations
In sum we have been left to ‘make our own arrangements’ if we want to protect ourselves against catching Covid. So what might this consist of?
2 Assessing and Avoiding Risks
2.i Assessing Risk
Many of us, particularly the clinically vulnerable and their households. have built up a good almost intuitive understanding of how to assess whether a situation is risky and what mitigations need to be in place, but as noted above this needs to be based on an up to date understanding of the basic science of COVID-19.
Data
In order to inform our assessments many of us where until 2023 making judgements based on the level of infection at any particular point in time. However, since the dismantling of more or less all data on the level of covid infections, including the ONS infection survey, this is no longer possible, particularly during the summer months when the authorities seem to assume that Covid-19 has disappeared. These data issues are discussed elsewhere on this website.
CO2 monitors

Given that there is next to no information provision about the safety of buildings we and many other clinically vulnerable families also use a CO2 monitor in order to guide our deployment of the behaviours and measures described in sections 2ii and 3 below. There are a variety of monitors on the market ranging in price from well under £50 to £199 and upwards. We initially bought a cheap model but we quickly began to doubt its accuracy. It also required recharging every 12 hours and was bulky to carry around. We subsequently invested in an SAF Aranet 4 air quality monitor for £199. This seems far more responsive to changing conditions, is small and easy to transport around and it is claimed that the batteries last for 4 years.

It has proved very useful to us in checking out the potential for virus transmission in various places we need to do to including vaccination pharmacies. It has also been helpful in educating us about safety levels inside the house.
Air quality is meant to be 400 ppm of CO2 outdoors and we aim to keep the air inside the house at below 700. If it goes above 900 we open a door or window.
People also regularly use monitors when flying. On many flights the readings go up to over 5000 ppm, sometimes higher, in the period just after boarding before the engines and the air filtration systems are switched on at which point readings fall dramatically.
2.ii Avoiding Risk
Many clinically vulnerable families deploy a range of behavioural methods in order to avoid or lower the risk of coming into contact with the virus in the first place based on our assessment of the risk.
My household has extensive experience of such measures which include the following. This may seem excessive if you are not clinically vulnerable, but at least some of it may be relevant if you wish to avoid Covid.
- avoiding indoor gatherings and doing contacts, classes, talks etc on zoom instead. This also includes working from home. We make extensive use of zoom and similar, I am even learning French via an on-line class;
- Avoiding gatherings altogether if you consider the people you are meeting are inflexible and do not respect your need to stay safe or it is not possible in other ways;
- Social distancing, both indoors and outdoors plus use a HEPA filter indoors as well as opening the windows (see section 3ii below);
- avoiding unnecessary face to face appointments such as medical appointments or having work people in the house or doing it by telephone. Where we do have people in the house to do necessary services or repairs we wear masks, have a HEPA on and leave the door open – even when it is sub zero outside!;
- Doing things first thing in the morning when the viral load in the air will be lower eg. Going to the garden centre early, seeking out the first dental appointment of the day, traveling on public transport at non peak times.
- challenging health and other providers, including schools about their safety measures – this is a fraught issue which many people struggle with, particularly since the withdrawal of the requirement to wear a mask in healthcare. There are groups on social media that have a number of ready made outline letter templates for different situations
- testing before key events and requiring others to test – but don’t necessarily trust the results of one LFT as it is possible that they may be becoming less accurate at detecting new omicron variants. See my forthcoming post on Testing for Covid-19.
- seeking out a Covid safe mobile hairdresser or other business person depending on your needs. I have been using a mobile hairdresser called Angela since August 2020. She deploys a range of mitigation measures set out in the following video which is helpful in setting out best practice.
3. Masks, local ventilation/air filtering, gadgets, potions, sprays
This section is about some of the various methods that can be deployed to avoid catching Covid even when, despite our best methods of avoiding it, we come into direct contact with it. It is important to note that the evidence on all of these techniques is far from perfect which is in part explained by the fact that they are all deployed in different ways (see discussion under masks below) and often in combination which means it is impossible to single out how effective each individual method is at preventing the spread of Covid. This is sometimes called the Swiss cheese approach!

3.i Masks
The most contentious but one of the most effective is for people to wear a mask. Yet the number of people wearing a face covering has dropped off to the extent that only a small minority wear one and in many cases these people have become a figure of fun for doing so (see note on assertiveness in the final section of this paper).
All of the evidence shows that masks can reduce the chances of catching the virus but the type of mask you and others wear, the level of ventilation (see section 3.ii below), your activities and the behaviour of others around you are all very important.
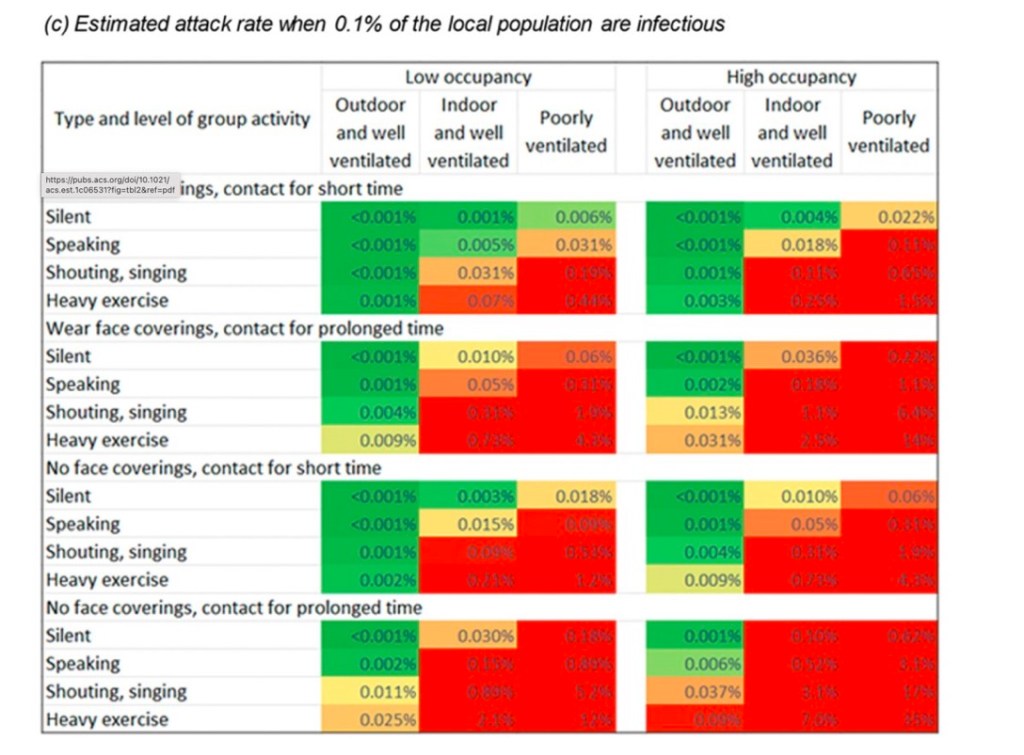
The table below from an article by Trish Greenhalgh and others summarises the situation very well. This research quantified how the different influences on transmission change your risk of getting sick: viral factors (transmissibility/prevalence), people factors (masked/unmasked, exercising/sitting, vocalising/quiet) and air-quality factors (indoors/outdoors, big room/small room, crowded/uncrowded, ventilated/unventilated). The researchers did this by carefully studying empirical data on how many people became infected in superspreader events where key parameters, such as the room size, room occupancy and ventilation levels, were well-documented and by representing how transmission happens with a mathematical model.
The type of mask you wear is also very important. Simple cloth masks or baggy blues type surgical masks may have been appropriate in 2020 when no other types of masks were available, but the virus has become far more innovative since then and the evidence suggests that a minimum of FFP2 masks (readily available and relatively cheap), or even better FFP3, should be the minimum. Also, it is important to be aware that non valved masks are best because they help protect others around you as well as you (a valved mask is only of benefit to you).

There is also strong evidence that masks that go all the way around your head such as the widely available 3M Aura are more effective than an ear loop mask. They are certainly more likely to pass a fit test. I personally prefer the Netherlands manufactured handanhy variant of this (bottom mask in photo) because I feel it gives me a better fit but they are more expensive and more difficult to buy in the UK, though the face mask store now sells them.
Of course the ideal way to know how much protection you are getting from your mask is to do a fit test. However, fit testing kits are very expensive and rather complicated to carry out . I have not bothered with fit testing in part because the type of mask I wear depends on the context and length of time I am going to be exposed. If I am going to the dentists and will need to slip my mask on and off or if I am popping into a shop briefly, for example, or if I am seeing my mobile hairdresser I tend to wear a FFP3 ear loop mask since one that goes round the head is clearly going to impede her work. However, if I go on a train/bus journey or accompany my husband to a medical appointment I tend to wear a wrap round the head handanhy.
There is of course a great deal of misinformation around about masks driven in part at least by people feeling they are an infringement on their ‘freedoms’.
One of the most damaging claims which received extensive coverage in the media is the Cochrane review co-ordinated by Tom Jefferson. Jefferson happens to work with the Brownstone Institute which has always been an extremely anti-mask, anti-vaxx right wing think tank”.
Nevertheless, it has been extensively reported that this study shows that face masks don’t work to the extent that many people now regard this as ‘common knowledge’. This is highly misleading as explained by the editor in chief of the Cochrane library who concludes that given the limitations in the primary evidence, ‘the review is not able to address the question of whether mask-wearing itself reduces people’s risk of contracting or spreading respiratory viruses.’
This is not surprising given that Cochrane reviews only ever take into account evidence from randomised control trials (RCT’s), and there are significant methodological reasons why randomised control methods are particularly challenging on this particular topic. Masks are a society wide intervention rather than a narrow medical intervention which is what RCT’s are most suited for. As we have seen above, the effectiveness of masks will depend on the societal context including how long they are worn for, where, whether everyone is wearing a mask, the type of mask, levels of infection etc.
Moreover, the paper mixes together studies that were conducted in different environments with different transmission risks. It also combines studies where masks were worn part of the time with studies where masks are worn all the time. And it blends studies that looked at Covid-19 with studies that looked at influenza. But mixing up COVID-19 with influenza is completely meaningless because they are very different illnesses; indeed, the pandemic game changer was when studies revealed that the SARS-CoV-2 could actually travel in smaller and lighter respiratory droplets that could hang in the air for much longer periods of time and could float for more than six feet. It is completely unlike flu which transmits via large droplets.
Out of the 78 papers analyzed in the review, only two actually studied masking during the Covid-19 pandemic. And both of those found that masks did protect wearers from Covid-19.”
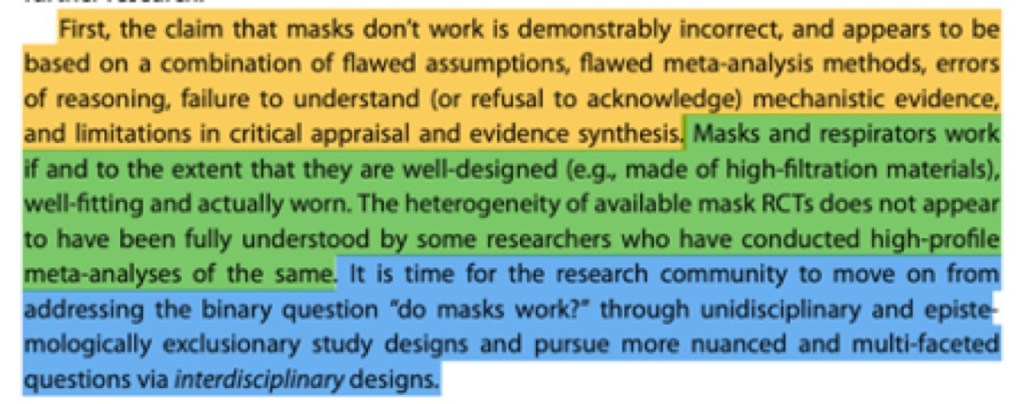
In conclusion the definitive meta analysis on masks was published in May 2024 by a team led by Trisha Greenhalgh. This shows conclusively that good quality masks work, concluding that we need to move on from the binary question of do masks work.
Before moving on from the subject of masks I need to briefly mention nose plugs. These a small plugs that you place up your nose – see photo. You need to insert them carefully and obviously dispose of them carefully and wash your hand afterwards.
They are meant to catch the virus before it reaches up into your nose but trials have demonstrated that they are, at best, 60% effective. Nevertheless some people take the view that they are better than nothing for situations where you can’t wear a mask (eg. The dentists) or where some would feel uncomfortable wearing one eg weddings.

Personally I find them uncomfortable as they make my nostrils feel very full and I do not recommend them.
The other type of barrier method is visors ie a plastic shield that covers the face. I don not know anyone who recommends them, as the sole means of protection, given that Covid is airborne and can creep in underneath the visor. Indeed, they have been likened to a chocolate fire guard!
3 ii Clean Air :Ventilation, air filters and wearables
We have already seen that Covid-19 transmits in smaller and lighter respiratory droplets than other types of virus and can hang in the air for much longer periods – sometimes hours if there is no ventilation. Good ventilation is therefore a very important weapon against Covid, used in conjunction with other measures, if possible.

Many other governments around the world recognise this and stress the importance of clean air in public and other buildings. The mega rich also recognise it. The pictures from the DAVOS 2023 meeting held in January were revealing in that a very strong air filtration system was in operation and HEPA filters were clearly visible in all the smaller meeting rooms.
Following on from this example, the fact that people in the UK are not rising up and demanding clean air in buildings such as hospitals and schools is a puzzle, particularly when you consider that the UK Houses of Parliament are one of the few public buildings with a proper air filtration system.
So, what can individual households do? The cheapest thing you can do is open windows and doors to get a draft through when there is anyone in the house or flat. We do this even when the temperature is minus 10 degrees outside – you just need to put a coat on!
We can see from the following table that the chances of catching Covid in a well ventilated setting where the CO2 level is lower than 800 will be far lower than where CO2 levels are high.

It is also a good idea to buy a HEPA filter strong enough to help to clean the air in a room. HEPAs are designed to remove particles from the air though claims made by some manufacturers about removing Covid particles completely may be exaggerated, there is research evidence to suggest they work. Many scientists assess them as being effective. They also have several other benefits such as reducing pollen and dust.
Following the King’s recent cancer diagnosis it is clear that the palace recognise the benefits of a HEPA filter even though they may not be well informed about the relative effectiveness of different models. The model on display in the following photograph will be familiar to many people as the most expensive and also least effective model according to Which!

There are a variety of models on the market starting from about £200. We have two Phillips machines which we bought 4 years ago due to major building works next door. We always have them on when there are any visitors in the house regardless of whether the windows are also open. It is important to read the manufacturers instructions about how to set them up and where to place them.

The Corsi- Rosenthal Box is a homemade filter box and is relatively cheap to make. It is often touted as the answer to providing every school classroom in the country with some level of filtration. It has been claimed that having a box on in a classroom reduces the incidence of COVID by 82%. Involving children in the building of boxes is also thought to have positive spin offs in educating them about air quality and following instructions to build something mechanical.
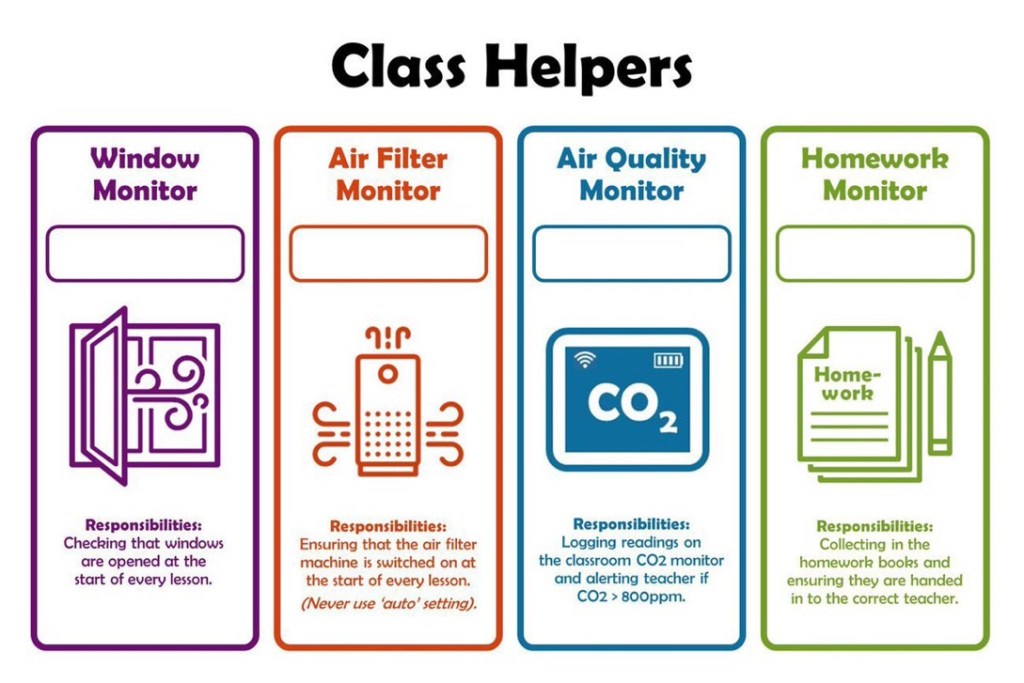
Some schools, particularly outside the UK have also developed methods to involve children actively in the operation of filters once they are up and running by building up a sense of responsibility for their operation – see diagram.
But what about when you are out and about? I recommend a small portable HEPA filter. These filters do not clean the entire room and are only effective if you hold them about one meter or so away from you.

Nevertheless, we carry one when traveling on public transport, going to medical appointments in places without adequate protections etc. We have a Smart Air QT3 purifier which is non intrusive and looks like a portable radio and costs less than £50.

The other type of device aimed at removing the virus in the air around you is a small wearable gadget which typically use ionizers and ionization technology. There are many brands on the market ranging from about £20 upwards.
Essentially, they generate ions which attach to pollutants or viruses in the air, giving them a static charge and cause them to drop to the ground. Manufacturers of traditional air purifiers like to try to discredit these devices, though it is true that there is no robust evidence on their effectiveness. Nevertheless, we have two Air tamers which we wear at the dentists.
3 iii Nose Sprays and Mouth Washes
We deploy both of these methods but particularly nose sprays in combination with other measures, particularly masks. Again, there is little to no robust evidence on their effectiveness.
There are a variety of nasal sprays on the market which fall into one of two types:
- sprays containing nitric oxide that claim to kill the Covid-19 virus whilst it is the nostril and prevent infection entering your body through the nasal passage. The best known brand is Enovid which is not available in the UK but can be obtained quickly and easily, if expensively, from a pharmacy in Israel. I have used it in the past but unfortunately it gives me a headache. However, many people use it regularly and have great confidence in it.
- The second type of spray trade under a variety of labels including Boots Dual defence, and Vicks First defence which do not make hefty claims about killing Covid but many people claim they can shorten the duration of illness or stop it developing. Another type of spray – NoriZite does make claims that it ‘coats the nasal cavity and creates a fast, long-lasting barrier against airborne virus particles including Covid-19’. Similar sprays include Viralise and BioSURE. I am sceptical about these hefty claims but these are my favourite sprays as they do not lead to side effects for me. However, I would never use them as the only method of defence.
As far as mouthwashes are concerned, those marked ‘CPC protect’ work on the theory that they de-activate any Covid-19 infection present in the human saliva. As far as I am aware they have not been tested in real life conditions but I tend to use it, particularly when going to the dentists, in combination with other measures. It has no side effects for me, is relatively cheap, I need to use a mouthwash and I take the view that anything is worth a try.
Again I would never use as a sole means of defence.
Concluding remarks
I am in the fortunate position of being retired and having enough resources to buy gadgets to help to protect us. I have also recently paid £65 for a private novavax vaccination because of the crazy position that although my husband is entitled to a free spring booster, I am not despite living at close quarters with him. I am aware that many people are in a worse position and, for example, are forced to go to workplaces without protective measures despite the dangers, and cannot afford to buy things like HEPA filters. There are no easy answers here except to say that there are measures that can be deployed relatively cheaply such as FFP2 masks, opening windows in houses, flats, cars and vans, offices etc, meeting outside, homemade HEPA’s and similar, and social distancing. There are also a variety of resources on line that aim to make it easier to raise concerns about the safety of workplaces and schools, for example.
The clinically vulnerable families group which I am active in are also campaigning hard for improvements.

I am also fully aware that behaviours such as practicing social distancing, wearing a mask, carrying a personal HEPA, saying no to meeting in indoor settings can attract abuse from others and is difficult for people, particularly those who are not naturally assertive or who are ill.
My impression is that people feel that these kinds of behaviours have become more common in the relatively recent past as the government, its agencies and most of the media are trying to airbrush anything to do with Covid under the carpet and pretend that everything is back to normal. See for example, my post on mask abuse and discrimination.
Incidents I have personally witnessed or heard others talk about range from sheer rudeness in the street, laughing and pointing in the supermarket, or more subtle indications of disapproval particularly around mask wearing. It also seems that polite refusals to meet up can be met by ‘gaslighting’ from others, including family members and friends. Common methods include calling people stupid, having blazing arguments, telling them to ‘get a life, making them feel guilty through to very nasty psychological manipulation eg. ‘I am vulnerable as well and I do x,y, & z’. The lack of respect for others and the sheer nastiness of all of this is very upsetting for many people, and for many this type of behaviour seem to peak around christmas time.
We have no way of knowing how many people who want to be careful have been bullied or gaslighted into taking risks they do not want to take. One hopes that it is not too many but I suspect it is quite high which is very sad given that people are effectively telling other people to place their lives or the lives of others at risk.
There are a variety of ways in which people can train themselves to be more assertive and stand up to bullying and there are on-line resources and private on-line groups of people who understand and who are happy to provide support.
We do not know what will happen next with Covid. One hopes that Covid will magically petter out or become milder, or that better vaccines and treatments come on stream that work for people with weak immune systems.
Alternatively, one hopes that the UK government and other governments suddenly see the light and implement the range of policies needed to reduce the spread and damage done by infections, do what is needed to treat and research long covid, or even simply provide up to date information to the general public – in other words tell the truth.
Nevertheless, we are where we are which is a considerable way from the vision outlined in the previous sentence. I hope this note is helpful to people, particularly the clinically vulnerable and their families in navigating the current situation.

Leave a comment